Research Article
Feasibility study on the evaluation of the effect of narrow-band CE-Chirp ASSR in the hearing field after hearing aid in hearing-impaired children

Wang Yonghua* and Xing Shuoyao
Zhejiang Chinese Medical University, Hangzhou, Zhejiang, China
*Address for Correspondence: Wang Yonghua, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, China, +86 13606626396; Email: [email protected]
Dates:Submitted: 28 June 2019; Approved: 11 July 2019; Published: 12 July 2019
How to cite this article: Yonghua W, Shuoyao X. Feasibility study on the evaluation of the effect of narrow-band CE-Chirp ASSR in the hearing field after hearing aid in hearing-impaired children. Adv Treat ENT Disord. 2019; 3: 007-011. DOI: 10.29328/journal.ated.1001007
Copyright License: © 2019 Yonghua W, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Abstract
Objective Study: Whether the narrow-band CE-Chirp ASSR test in the sound field is an objective evaluation method for the hearing aid compensation effect, and whether there is a difference in children with different hearing loss levels.
Methods: 39 children (67 ears) wearing full digital hearing aids with good rehabilitation effect and ability to cooperate with behavioral audiometry were selected. The narrow-band CE-Chirp ASSR test group in the sound field was set as the experimental group, and the sound field behavioral audiometry after hearing aid was set as the control group. According to the degree of hearing loss, it was divided into moderate hearing loss group, severe hearing loss group and extremely severe hearing loss group. The difference between test results of experimental group and control group was compared.
Results: There were no significant differences between the experimental group and the control group in the moderate hearing loss group and the extremely severe hearing loss group at 0.5, 1, 2, and 4kHz (P > 0.05). The results of the experimental group and the control group in the severe hearing loss group, There was no significant difference at 0.5, 1, 2kHz (P > 0.05), there was a significant difference at 4kHz (P < 0.05), and the mean difference was - 6.4dB HL. When the degree of hearing loss was not grouped, there was no significant difference between the experimental group and the control group at 0.5, 1, 2kHz (P > 0.05), 4kHz was significantly different (P < 0.05), and the mean difference was -3.2dB HL.
Conclusion: It is clinically feasible to evaluate the hearing aid compensation effect of the narrow-band CE-Chirp ASSR in the hearing-impaired children. The grouping according to the degree of hearing loss can be more accurate in evaluating the hearing aid compensation effect. The narrow-band CE-Chirp in the sound field of children with moderate and very severe hearing loss ASSR results can be directly used to assess the hearing aid compensation effect, while children with severe hearing loss need to apply correction values at 4kHz.
Introduction
The early intervention method for early detection of hearing-impaired children is to fit the hearing aid. If the hearing aid is used for 3-6 months, the effect cannot meet the language development needs. The cochlear should be implanted as soon as possible. Therefore, it is important to accurately evaluate the hearing aid effect and choose the optimal intervention method in the early stage [1,2]. At present, the effect of hearing aids for hearing-impaired children is assessed by behavioral audiometry, but the results are affected by the intelligence level, coordination level, psychological status of the hearing-impaired children and the technical level of the inspectors [3,4]. Therefore, finding an effective objective assessment method for post-hearing rehabilitation is an urgent problem to be solved. Chirp ASSR is a technology that is induced by Chirp sound and incorporates multi-frequency sound and full spectrum detection engines. By simultaneously giving multiple frequencies of stimuli to both ears, and performing statistical analysis on the obtained multiple harmonics, the presence of ASSR is detected by the difference between harmonic frequencies and other frequencies. In this study, the narrow-band CE-Chirp ASSR was used to test the response threshold of children with moderate, severe and severe hearing loss in the sound field and the hearing threshold after behavioral audiometry. The test method was used to evaluate whether the hearing aid compensation effect was evaluated. This is important for selecting a precise rehabilitation strategy and assessing the rehabilitation effect after hearing aids.
Materials and Methods
Test subject
39 children with sensorineural hearing loss who were able to cooperate with behavioral audiometry with a full-digital behind-the-ear hearing aid (a total of 67 ears, grouped in ears), 22 males and 17 females, aged 2-7 years, the average age is 3.36±1.50 years old. Before the inclusion of the subject, the purpose and process of the experiment have been communicated to the guardian of the child and their consent has been obtained. The World Health Organization WHO-1997 stipulates that the average hearing at four frequencies of 0.5, 1, 2, and 4kHz is 41-60dB HL for moderate hearing loss, 61-80dB HL for severe hearing loss, and >80dB HL for severe hearing loss. Subjects were divided into moderate hearing loss group, severe hearing loss group and very severe hearing loss group according to this standard. All subjects tested the narrow-band CE-Chirp ASSR and behavioral audiometry under the sound field. The test sequence was based on random principle. The narrow-band CE-Chirp ASSR under the sound field was set as the experimental group. The hearing-detection behavior of the hearing-impaired children in this group was the control group.
Test steps and methods
Medical history collection: Hearing screening of newborns, time of hearing aid intervention, situation of language training and rehabilitation, history of otitis media, family history of deafness, and exclusion of children with hearing impairment such as mental and intellectual abnormalities.
Conventional otology examination: The external auditory canal and tympanic membrane were examined to confirm that the subject had no abnormalities in the external auditory canal that the tympanic membrane was intact and the marking was clear.
Acoustic impedance test: Check the bilateral tympanogram is “A” type.
Otoacoustic emission: All subjects underwent otoacoustic emission examination to exclude post-cochlear lesions.
Sound field calibration: Behavioral audiometry is performed in a standard soundproof room using GSI’s Audiostar Pro audiometer and ER-3A insert earphones. Sound field setting: the angle between the speaker and the sagittal plane of the subject is 45°, the center of the speaker is aligned with the external auditory canal, the distance is 1m and at the same horizontal plane. The sound field calibration is based on the national standard GB/T4854.7-2008, and the unit isdB HL. The narrow-band CE-Chirp ASSR under the sound field uses the Danish International Hearing Company Eclipse 25 objective hearing test platform, record the narrow-band CE-Chirp stimuli (stimulus rate 90Hz) of 0.5, 1, 2, 4kHz in the ASSR test system with a sound card and import it into the “Huier Hearing Test Software”, connect the amplifier and speakers. Sound field setting: The speaker is facing the subject’s head, at an angle of 0° to the subject’s lying position, at a distance of 0.6 m and at the same level. The sound system tests the hearing impaired subject for biological calibration during the development phase, and the electroacoustic engineer calibrates the sensor (speaker) in dB HL.
Behavioral audiometry: Confirm that the hearing aid is working properly before the test and the frequency shift noise reduction function is not turned on. Test ear wear hearing aid, opposite ear plus sponge anti-noise earplugs. Select visual reinforcement or game audiometry based on the subject’s age and behavioral ability, establish conditionalization, and ensure that the rules are fully understood and the test begins. The minimum intensity of more than two reliable responses is defined as the hearing threshold, and the hearing threshold of 0.5, 1, 2, 4kHz is obtained. Remove the hearing aid for 30 minutes, and then use the insert earphone to measure the bare ear threshold of 0.5, 1, 2, 4kHz.
Narrow-band CE-Chirp ASSR test under sound field: The test is carried out in an electromagnetic shielding room. The sleep deprivation method allows the hearing-impaired child to enter a natural sleep state, and 10% chloral hydrate (0.5 ml/kg) is orally administered to a hearing-impaired child who cannot sleep well. The recording electrode is placed in the middle of the forehead close to the hairline, the ground electrode is placed at the base of the nose, and the reference electrode is placed in the left and right mastoids. The impedance of all electrodes is <5kΩ, the impedance between the electrodes is <3kΩ, the stimulation frequency is 90Hz, and the artifact rejection level is ±40μV. Using the single-ear single-frequency test, the “Huier Hearing Test Software” gives the narrow-band CE-Chirp stimuli of each frequency through the speaker, and the tested ear wears the hearing aid (the settings of the hearing aid are the same as those of the behavioral listening), and the opposite ear add sponge anti-noise earplugs, use the 5 to 10 method to find the post-hearing response threshold for each frequency.
Statistical method: The paired sample T-test was used for the data of SPSS19.0 software. P < 0.05 was considered statistically significant.
Results
Moderate hearing loss group uses the experimental group and the control group test method to evaluate the hearing aid compensation effect
It can be seen from table 1 that there is no significant difference in the test results of the experimental group and the control group with moderate hearing loss at 0.5, 1, 2, and 4kHz (P = 0.317, 0.111, 0.052, 0.511, P > 0.05). The application of the narrow-band CE-Chirp ASSR in the sound field to evaluate the hearing aid compensation effect of children with moderate hearing loss can achieve the same accuracy as behavioral audiometry at 0.5, 1, 2, 4kHz.
| Table 1: Moderate hearing loss group uses the experimental group and the control group test method to evaluate the hearing aid compensation effect (dB HL). | |||
| Frequency (kHz) | Quantity (n) | Post-hearing response threshold and hearing aid threshold (dB HL) | |
| Experimental Group | Control Group | ||
| 0.5 | 16 | 30.3±12.0 | 32.8±8.2 |
| 1 | 16 | 29.4±6.6 | 31.3±5.6 |
| 2 | 16 | 31.3±13.2 | 36.3±10.9 |
| 4 | 16 | 29.3±11.9 | 31.0±7.4 |
| Note: Comparison between experimental group and control group, *P<0.05 | |||
Severe hearing loss group uses the experimental group and the control group test method to evaluate the hearing aid compensation effect
It can be seen from table 2 that there is no significant difference in the 0.5, 1, 2kHz between the experimental group and the control group of children with severe hearing loss (P = 0.755, 0.484, 0.311, P > 0.05), and there is a significant difference at 4kHz (P = 0.002, P < 0.05), mean difference is -6.4dB HL. The application of the narrow-band CE-Chirp ASSR in the sound field to assess the hearing aid compensation effect of children with severe hearing loss can achieve the same accuracy as behavioral audiometry at 0.5, 1, 2kHz, and the correction value needs to be applied at 4kHz.
| Table 2: Severe hearing loss group uses the experimental group and the control group test method to evaluate the hearing aid compensation effect (dB HL). | |||
| Frequency (kHz) | Quantity (n) | Post-hearing response threshold and hearing aid threshold (dB HL) | |
| Experimental Group | Control Group | ||
| 0.5 | 24 | 38.1±13.5 | 39.0±8.5 |
| 1 | 25 | 38.2±9.0 | 39.6±7.5 |
| 2 | 24 | 39.6±13.0 | 41.9±7.2 |
| 4 | 21 | 39.5±13.9* | 46.0±9.2 |
| Note: Comparison between experimental group and control group, *P < 0.05 | |||
Extremely severe hearing loss group uses the experimental group and the control group test method to evaluate the hearing aid compensation effect
It can be seen from table 3 that there is no significant difference in the test results of the experimental group and the control group of children with extremely severe hearing loss at 0.5, 1, 2, and 4kHz (P = 0.368, 0.538, 0.102, 0.509, P > 0.05). The application of the narrow-band CE-Chirp ASSR in the sound field to evaluate the hearing aid compensation effect of children with extremely severe hearing loss can achieve the same accuracy as behavioral audiometry at 0.5, 1, 2, 4kHz.
| Table 3: Extremely severe hearing loss group uses the experimental group and the control group test method to evaluate the hearing aid compensation effect (dB HL). | |||
| Frequency(kHz) | Quantity() | Post-hearing response threshold and hearing aid threshold dB HL) | |
| Experimental Group | Control Group | ||
| 0.5 | 25 | 46.0±10.3 | 48.0±9.2 |
| 1 | 26 | 47.7±9.8 | 46.5±8.9 |
| 2 | 26 | 51.2±10.3 | 48.7±9.9 |
| 4 | 23 | 52.6±13.6 | 53.9±9.4 |
Note: Comparison between experimental group and control group, *P<0.05 |
|||
When the degree of hearing loss was not grouped, the experimental group and the control group test method evaluate the hearing aid compensation effect
As can be seen from table 4, there was no significant difference between the experimental group and the control group at 0.5, 1, 2kHz (P = 0.230, 0.623, 0.376, P > 0.05), and there was a significant difference at 4kHz (P = 0.010, P < 0.05). The mean difference is -3.2dB HL. It is indicated that the narrow-band CE-Chirp ASSR and the behavioral audiometry difference in the sound field of children with different hearing loss levels are different, and need to be researched and applied in groups, especially 4kHz.
| Table 4: When the degree of hearing loss was not grouped, the experimental group and the control group test method evaluate the hearing aid compensation effect (dB HL). | |||
| Frequency(kHz) | Quantity(n) | Post-hearing response threshold and hearing aid threshold(dB HL) | |
| Experimental Group | Control Group | ||
| 0.5 | 65 | 39.2±13.3 | 40.9±10.5 |
| 1 | 67 | 39.8±11.3 | 40.3±9.6 |
| 2 | 66 | 42.1±14.3 | 43.2±10.4 |
| 4 | 60 | 42.0±16.1* | 45.3±12.6 |
| Note: Comparison between experimental group and control group, *P<0.05 | |||
Discussion
Development and clinical application of Chirp stimulation
Chirp stimulation is also called chirped pulse sound. The phase characteristic is that the low-frequency sound is emitted early, and the high-frequency sound is emitted late, so that more nerve fibers are synchronously discharged, increasing the reaction speed and amplitude, and shortening the detection time [5-7]. With the development of Chirp stimulation signals, Chirp ASSR has been widely used in China [8]. A number of studies [9-13] show that narrow-band CE-Chirp ASSR has good accuracy and reliability in objective hearing evaluation. The narrow-band CE-Chirp used in this study is to decompose the wide-band CE-Chirp sound into four frequency components centered at 0.5, 1, 2, and 4kHz, and has good frequency specificity. At the same time, the synchronizing of the auditory nerve caused by the delayed wave motion of the cochlea is overcome. The waveform is shown in figure 1.
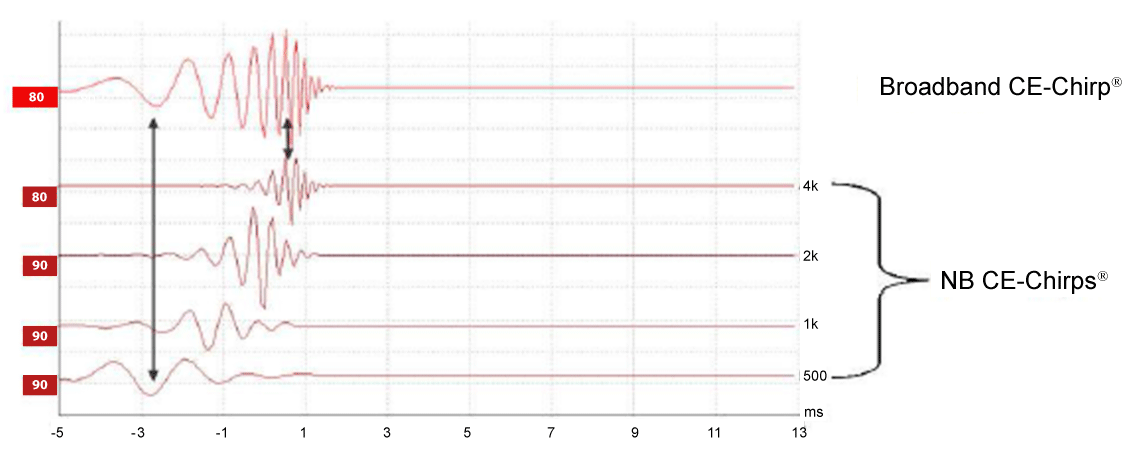
Figure 1: Broadband CE-Chirp and narrowband CE-Chirp waveforms.
Narrowband CE-Chirp ASSR under sound field
The Eclipse 25 objective hearing test platform used in this experiment works on the principle of detecting the phase and amplitude values of the first 6-8 harmonics from the changing biological noise and noise floor, and analyzing the 90 Hz fundamental harmonics and higher harmonics such as 180Hz, 270 Hz, etc. The response amplitude at the 90 Hz fundamental harmonic is the highest. As the number of harmonics increases, the response amplitude decreases. Compared with the single sample test method in which the traditional ASSR only analyzes the first harmonic, this new analysis method can improve the signal-to-noise ratio and obtain more optimized results [14]. Current research suggests that the origin of ASSR is related to the modulation frequency. When the stimulation rate is higher than 70 Hz, the ASSR is a steady-state response from the brainstem, which is unaffected by attention, arousal, and sleep [15]. In this study, the 90Hz stimulation rate was used, and the acoustic amplification of the hearing aid was uploaded to the brainstem [16], which laid the theoretical foundation for nerve conduction in the ASSR test under the sound field.
The experimental subjects were 39 hearing-impaired children with good auditory response, good rehabilitation effect and good performance of behavioral audiometry. The results obtained by the matching test are analogized to the evaluation of the hearing aid compensation effect of hearing-impaired children who cannot cooperate with behavioral audiometry. For hearing-impaired children who can obtain behavioral audiometry results, the electrophysiological threshold test results after hearing aids are obtained, and the subjective and objective test results are mutually verified, which has more scientific guiding significance [17].
Previous studies have pointed out that the ASSR low-frequency response correlation is worse than the high-frequency, which is presumed to be due to the fact that the hair cell and basement membrane near the volute are more synchronic than the volute, and the ASSR amplitude of the low-frequency signal is lower than the higher frequency signal [18,19], or the subject can’t completely relax or go to sleep in a short time, it is difficult to get a higher signal to noise ratio, which has the greatest impact on the low frequency. There were no significant differences between the experimental group and the control group in the low frequency of children with different hearing loss in this experiment. Probably because the subjects are in deep sleep state when testing the narrow-band CE-Chirp ASSR under the sound field, the EEG interference is small and the signal-to-noise ratio is high. During the test, the subject sometimes has sudden awakening or EEG interference. At this point, the test should be suspended, and the test should be repeated after it falls asleep again. The hearing-impaired child who cannot enter deep sleep again will be tested again within one week.
The results of this experiment should pay attention to the following problems in clinical application: 1. The hearing aid turns off the frequency shift noise reduction function in advance, otherwise it may affect the test result. 2. Exclusion of the ASSR electrophysiological response threshold and hearing-impaired children with mental and intellectual abnormalities in the bare ear, children with hearing impairment who have severe hearing loss or other developmental abnormalities should carefully use the narrow-band CE-Chirp ASSR in the sound field to evaluate the hearing aid compensation effect. 3. The results of this experiment are applicable to children with sensorineural hearing loss. It is not clear whether it is suitable for hearing-impaired children with middle ear lesions and posterior fossa lesions. 4. The conditions and layout of electromagnetic shielding rooms in different hearing centers are different. It is recommended to establish corresponding correction values for each hearing center to play a better guiding role in clinical application.
In summary, the narrow-band CE-Chirp ASSR under the sound field has clinical application value as an objective hearing aid evaluation method. For young children with moderate, severe and extremely severe sensorineural hearing loss, the application is based on the degree of hearing loss, children with severe hearing loss apply correction values at 4kHz, and children with moderate and extremely severe hearing loss do not need to apply correction values. It can achieve the same accuracy as behavioral audiometry, and can timely understand the compensation effect and functional status of hearing aids for hearing-impaired children, and help hearing-impaired children to choose the optimal intervention strategy to obtain the best rehabilitation effect.
Outlook
The single-ear single-frequency test method of this experiment takes a long time and the efficiency is not high enough. If you can explore a multi-frequency sound mode under the sound field, improve the test efficiency and shorten the test time, it is more conducive to clinical application. In addition, children with special hearing loss need to turn on the frequency shift function of the hearing aid. If we can study whether the narrow-band CE-Chirp ASSR in the sound field can effectively evaluate the digital hearing aids with the frequency shifting function enabled, it can greatly help this part of the hearing-impaired children.
References
- Jianhua Z, Xiaobing L, Lin L. A Comparison of Aided Hearing Thresholds by Behavioral Audiometry and Auditory Steady-state Response in Sound Field. Chinese Scientific Journal of Hearing and Speech Rehabilitation. 2011; 6: 26-29.
- Tingting F. Relevant Problems about the application of ASSR in the auditory diagnosis. Medical Equipment. 2012; 25: 22-24.
- Sha L, Ruijuan D. Behavioral Audiometry in Children. Journal of Audiology and Speech Pathology. 2017; 25: 219-220.
- Jinxiao Z, Ling L, Wendi S. Correlative analysis of octave band CE-Chirp ABR and behavioral auditory in children with hearing loss. Chinese Archives of Otolaryngology-Head and Neck Surgery. 2018; 25: 83-85.
- Sturzebecher E, Cebulla M, Elberling C, Berger T. New efficient stimuli for evoking frequency specific auditory steady-state responses. J Am Acad Audiol. 2006; 17: 448. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/16866006
- Xiaoya W, Renzhong L, Jun L, Wen RJ, Zou Y, et al. Correlation between chirp auditory brainstem response and behavioral hearing threshold in children. Chinese Journal of Otorhinolaryngology Head and Neck Surgery. 2009; 3: 190-191. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/19558855
- Elberling C. Don M. Cebulla M, Stürzebecher E. Audirtory steady-state responses to chirp stimuli based on cochlear traveling wave delay. J Acoust Soc Am. 2007; 122: 2772-2785. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/18189568
- Wenting L, Jiangshun S, Jinghua X. Correlation between Evoked Auditory Steady State Response(ASSRs) and Pure Tone Audiometry(PTA) in Children. Chinese Journal of Otology. 2016; 14: 191-194.
- Shi Wei, Guo Wei, Wang Qiuju. NB CE-Chirp ASSR Application in Infant Hearing Screening and Diagnosis. Journal of Audiology and Speech Pathology. 2011; 19: 7-10.
- Qiming L, Jinming Z, Lizi Q. Analysis of the correlation between CE-Chirp ASSR and the behavioral hearing thresholds. The Journal of Practical Medicine. 2012; 28: 2522-2555.
- Fanqin W, Zhaoqun L, Guanping Z. Correlation between Frequency-Specific Chirp Auditory Steady-State Responses and Pure Tone Audiometry in Adults. Chinese Journal of Otology. 2012; 10: 451-454.
- Fanqin W, Guanping Z, Zhaoqun L. Correlation between Frequency-Specific Chirp Auditory Steady-State Responses and Pure Tone Audiometry in Children. Chinese Journal of Otology. 2014; 12: 235-238.
- Yuan L, Xiaohuan B, Yi S. Narrow Band CE-Chirp ASSRs and Conventional ASSRs in Children with Profound Hearing Loss. Chinese Journal of Otology. 2018; 16: 340-343.
- Cebulla M, Sturzebecher E, Elberling C. Objective detection of auditory steady-state responses: comparison of one-sample and q-sample tests. J Am Acad Audiol, 2006; 17: 93-96. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/16640063
- Picton TW, John MS, Dimitrijevic A. Human auditory steady-stated responses. Int Journal Audiol. 2003; 42: 177.
- Xingqi L, Qiuju W. Fundamental and Application of Auditory Evoked Response. Beijing: People's Military Medical Publisher. 2015; 211-217.
- Daofeng N. American Academy of Audiology Clinical Practice Guidelines: Pediatric Amplification. Chinese Scientific Journal of Hearing and Speech Rehabilitation. 2014; 12: 170-173.
- Chuling L, Shujuan T, Xianglin L. Relationship between Evoked Auditory Steady-state Responses and Pure Tone Audiometry in Children with Different Levels of Hearing Loss. Journal of Audiology and Speech Pathology. 2017; 25: 591-593.
- Wenbo J, Weiqing X. Test on Auditory Steady-state Responses of Normal-hearing Adults. Anhui Medical and Pharmaceutical Journal. 2010; 14: 668-670.