Research Article
Changes in the frequency and intensity of Tinnitus using the Suppressive Noise Spectrum

Ming Zhang1-4*, Alysia Jeske1 and Sarah Young1
1Communication Sciences & Disorders, University of Alberta, Edmonton, Alberta, Canada
2Surgery-Otolaryngology, University of Alberta, Edmonton, Alberta, Canada
3Audiology, Glenrose Rehabilitation Hospital, Edmonton, Alberta, Canada
4Communication Disorders, Louisiana State University Health Sci Center, New Orleans, USA
*Address for Correspondence: Ming Zhang, M D, Ph.D, LSUHSC, 1900 Gravier St 9C3, New Orleans, USA 70112, E-mail: [email protected]
Dates: Submitted: 10 June 2017; Approved: 20 July 2017; Published: 21 July 2017
How to cite this article: Zhang M, Jeske A, Young S. Changes in the frequency and intensity of Tinnitus using the Suppressive Noise Spectrum. Adv Treat ENT Disord 2017; 1: 006-012. DOI: 10.29328/journal.ated.1001002
Copyright License: © 2017 Zhang M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Tinnitus; Customized Sound; Sound Therapy; Rehabilitation; Outcomes; IOWA Tinnitus; Handicap Questionnaire (THQ)

ABSTRACT
Objective:To report findings of improvement in patient tinnitus intensity and changes in frequency using a novel suppressive noise spectrum.
Design: Single-subject; each subject served as his or her own control. Each patient received treatment, and changes were measured over time.
Setting: Tertiary referral via university otolaryngology and hospital audiology as well as audiology clinics in the region.
Patients: Fifteen tinnitus ears in 8 patients.
Interventions: Therapeutic and rehabilitative.
Main Outcome Measures:: Tinnitus frequency, tinnitus intensity, and tinnitus questionnaire.
Results (Findings): After 3 months of exposure to the customized suppressive noise spectrum therapy, patients showed a shift in tinnitus frequency in addition to a significant decrease in tinnitus intensity from the pre-treatment to post-treatment condition (p < 0.05). Typically, improvement was gradual based on comparing 3 sets of data collected at baseline, 1.5 months and 3 months.
Conclusion: Using suppression in tinnitus is novel. Based on our findings, using a customized suppressive noise spectrum is effective in shifting the frequency, reducing the intensity of subjective tonal tinnitus, and improving the handicap based on THQ test. From this seminal report, factors related to maximizing its effectiveness (e.g., length of listening time, level of hearing loss, and application for alternative tinnitus types) may be considered for future research.
INTRODUCTION
Negative Impact
Approximately 10 to 15% of adults experience tinnitus severe enough to require medical service [1-3]. Up to 6% of tinnitus sufferers have incapacitating symptoms [2]. Tinnitus can affect emotions [4], attention [5], cognition [5] and working memory [6], as well as cause anxiety, depression, hyperacusis, insomnia and hearing loss [1,3] resulting in decreased quality of life [7].
No Cure
While a variety of therapies may provide relief and reduce symptoms [8-11], no cure has been identified [12,13]. To explore a new approach, we created a novel suppressive noise spectrum to reduce tinnitus intensity, which also shifted tinnitus frequency in some patients. To our knowledge, no such report has been identified.
METHODS
Participants
Eight patients presented with subjective tonal tinnitus, and met inclusion criteria (inclusion: ≥18 years old, tonal tinnitus >6 months, undiagnosed cause of tinnitus; exclusion: non-tonal tinnitus, severe hearing loss, using other treatment, unable to use earphones, significant depression). The Institutional Review Board approved the ethics of this report. There were several patients who attended the first session but later withdrew. At 0.5, 1, 2, 4, and 8 kHz, the mean hearing threshold was 28.5 dB HL for right ears and 35.8 dB HL for left ears. The majority of patients had presbycusis or a noise-induced hearing loss pattern. Additional patient clinical variables are presented in Table 1.
| Table 1: Summary of selected clinical variables of all patients. | ||
| clinical variables | ||
| gender | male (n = 5) female (n = 4) |
|
| tinnitus duration | 1-3yrs (n = 4) 5+yrs (n = 2) 10+yrs (n = 2) |
|
| possible causes | presbycusis noise-induced psychological trauma middle ear infection Ramsay Hunt Syndrome hereditary unknown cause |
|
| mean | standard deviation | |
| age (yrs) | 60 | 12.88 |
| hearing threshold (dB) | R: 28.5 L: 35.75 |
R: 16.48 L: 19.00 |
| tinnitus frequency (Hz) | 4139.7 | 2032.80 |
Design and Application of Novel Suppressive Noise Spectrum
Using a single-subject design for a group of patients, we compared data collected at baseline, 1.5 months, and 3 months.
As previous tinnitus studies used a t-test for statistical analysis [4,10,14], we used the same to compare pre-, mid-, and post-treatment data.
Tinnitus frequencies and intensities were identified using a Lenovo IdeaPad U410 Ultrabook Laptop and Bio-logic insert earphones with foam tips. A program was created to produce tones from 15 to 15000 Hz with a volume control of 0 to 100. Patients matched the computer-produced tone with their tinnitus frequency and intensity.
The IOWA Tinnitus Handicap Questionnaire (THQ) was also used.
The suppressive noise spectrum, in short, was created and customized to each patient to create the audio file. Suppressive frequencies and intensities were used to shape the white noise spectrum. In detail, a two-tone suppression mechanism was used. The intensity and frequency below and above patient tinnitus frequencies (i.e., near one octave and half-octave) were identified to suppress the tinnitus effectively. The noise is white noise that has been modified. The spectrum of the white noise is relatively flat. The modification uses a non-flat spectrum to modify the white noise, so that the spectrum is no longer flat. Because the noise is modified by a spectrum that differs from the spectrum of white noise, this spectrum-modified noise is termed as a suppressive noise spectrum. The spectrum of noise is determined by both patient and researcher. The researcher determined with patients the initial frequencies and intensity of both the tinnitus and the sound that can suppress the tinnitus. Based on this initial determination, the researcher created the spectrum noise. Listening to the spectrum noise is expected to suppress the tinnitus.
Our protocol required patients to listen for 2 hours per day. The spectrum noise were modified at 1.5 months based on updated patient data.
To verify the actual usage time, a time log note was given to patients to record how long they listened to the spectrum noise in 0.25, 0.5, 1.0, 1.5, and 2.0 hour increments.This therapy spectrum was expected to reduce tinnitus intensity and remap the cortex of the tinnitus spectrum (e.g., shift frequencies).
To our knowledge this suppressive noise spectrum is novel with no previous literature reporting these methods and findings.
RESULTS
Tinnitus Intensity
Intensity across all patients and sessions was normalized to volume control value 0-100 (see Methods). Results of a paired-samples t-test showed that after 3 months of exposure to therapy, patients experienced a significant decrease in tinnitus intensity from baseline (M=43.4, SD=32.4) to the post-treatment condition (M=22.5, SD=10.6, p<0.05) (Table 2). A one-tailed t-test was used as a reduction was expected. The mean decrease in intensity was 35% (SD=33.2), with a mean listening time of 185.1 hours (SD=74.2 hours). When patients were grouped by age, both groups experienced significant reductions in intensity [Table 3 (p<0.05)].
| Table 2: Results for Tinnitus Intensity, Tinnitus Frequency (Hz), and THQ Scores. | ||||||||||||
| Pre-test (1) | 1.5 Months (2) | 3 Months (3) | p-value | |||||||||
| Outcome | M | SD | M | SD | M | SD | ||||||
| 1-2 | 2-3 | 1-3 | ||||||||||
| Intensity | 43.39 | 32.42 | 25.83 | 12.73 | 22.49 | 10.62 | *< 0.05 | > 0.05 | *< 0.05 | |||
| Frequency | 4139.68 | 1811.04 | 3766.11 | 2517.16 | 3653.96 | 2560.38 | > 0.05 | > 0.05 | > 0.05 | |||
| Q-Positive | 50 | 37.34 | 59.37 | 38.86 | 71.25 | 32.27 | > 0.05 | > 0.05 | *< 0.05 | |||
| Q-Negative | 31.93 | 23.59 | 30.40 | 24.71 | 29.33 | 23.76 | > 0.05 | > 0.05 | > 0.05 | |||
| Table 3: Descriptive Statistics and t-test Results for Tinnitus Intensity by Age. | ||||||||||
| Pre-test (1) | 1.5 Months (2) | 3 Months (3) | p-value | |||||||
| Age Range | M | SD | M | SD | M | SD | ||||
| 1-2 | 2-3 | 1-3 | ||||||||
| 44-63 | 23.18 | 11.45 | 18.72 | 13.39 | 16.96 | 9.43 | *< 0.05 | > 0.05 | *< 0.05 | |
| 64-83 | 61.07 | 34.99 | 32.06 | 11.32 | 27.33 | 9.59 | *< 0.05 | > 0.05 | *< 0.05 | |
Of the 7 patients with bilateral tinnitus, 71% (n=5) showed a reduction in both ears and 29% (n=2) in 1 ear. The patient with unilateral tinnitus in the right ear experienced a 47% decrease from the first to second session, but an increase of 13% from the first to final session.
Tinnitus Frequency
Seven patients experienced a decrease in tinnitus frequency approaching statistical significance in the left ear [Table 4 (p=0.055)]. This was not statistically significant in the right ear (p>0.05).
| Table 4: Descriptive Statistics and t-test Results for Right Ear and Left Ear Intensity and Frequency (Hz). | |||||||||
| Pre-test (1) | 1.5 Months (2) | 3 Months (3) | p-value | ||||||
| Outcome | M | SD | M | SD | M | SD | |||
| 1-2 | 2-3 | 1-3 | |||||||
| R Ear Intensity | 27.12 | 12.08 | 23.89 | 14.04 | 22.98 | 11.19 | > 0.05 | > 0.05 | > 0.05 |
| R Ear Frequency | 3707.20 | 2013.33 | 3771.58 | 2954.37 | 3698.47 | 3050.12 | > 0.05 | > 0.05 | > 0.05 |
| L Ear Intensity | 62 | 39.07 | 28.06 | 14.10 | 21.93 | 19.80 | *< 0.05 | *< 0.05 | *< 0.05 |
| L Ear Frequency | 4633.95 | 1545.81 | 3759.86 | 2145.02 | 3606.09 | 2106.40 | > 0.05 | > 0.05 | #0.055 |
| *p < 0.05; # p = 0.055, two-tailed test and very close to 0.05 (when using one-tailed test, p < 0.05). | |||||||||
The mean pre-treatment tinnitus frequency was 4139.7 Hz (SD=1811 Hz), which decreased an average of 18% (SD=41.1). Of the 7 patients with bilateral tinnitus, 43% (n=3) showed a frequency reduction in both ears, 43% (n=3) in 1 ear, and 14% (n=1) experienced an increase in both ears. The patient with unilateral tinnitus also showed a frequency reduction.
IOWA Tinnitus Handicap Questionnaire (THQ)
The THQ consists of 2 Q-Positive questions (“I think I have a healthy outlook on tinnitus” and “I have support from my friends regarding tinnitus”), where scores closer to 100 indicate improvement, and 27 Q-Negative questions (related to physical, social and emotional health), where scores closer to 0 indicate improvement.
Improvement was significant for Q-Positive questions [Table 2 (p<0.05)] moving from 50 (SD=37.3) to 71.3 (SD=32.3). Q-Negative scores also improved, although not significantly (p>0.05).
DISCUSSION
This is the first report of suppressive noise spectrum therapy. Our data demonstrates suppressive noise spectrum therapy is effective in shifting tinnitus frequencies and reducing the intensity of subjective tonal tinnitus. Three patients reported their tinnitus to intermittently “drop out” and temporarily disappear. A next step would be to trial this method with those who experience forms of non-tonal tinnitus.
The following discussion focuses on our findings, as well as contributing factors such as left versus right ear receptiveness to treatment, listening period, and limitations.
Novel Suppressive Noise Spectrum
The suppressive noise spectrum is the novel contribution of this report as no literature was identified to report 1) using a two-tone suppression mechanism, 2) creating a suppressive noise spectrum with such parameters, 3) customizing the sound spectrum to each patient, 4) using this noise spectrum in treatment, and 5) using this noise spectrum to modify tinnitus intensity and frequency.
Improving Tinnitus Frequency
For patients with greater hearing loss in the left ear (n=5), tinnitus frequency consecutively lowered each visit. In our initial data we noticed shifts in tinnitus frequencies, which was supported by our two-tailed analysis (p=0.055). The data pointed more strongly to a lowering of tinnitus frequencies; thus, a one-tail analysis was performed to confirm (p<0.05). A number of patients reported lower tinnitus frequencies (below speech frequencies) were more tolerable. Therefore, this lowering of frequency may be an additional benefit of this treatment.
It is possible that as louder high frequencies are treated, softer low frequencies become more apparent. Low frequencies may also be suppressed by high frequencies, but emerge after high frequencies are treated. We consider our data and discussions here as frequency remapping up to the cortical level, and also as a support to what has previously been described related to remapping the cortex [15].
Subjective Survey Results
Our THQ data supported the results of tinnitus intensity reductions. Q-Positive data showed a statistically significant improvement (p<0.05). Q-Negative scores were improved although not yet reaching significance. Q-Negative data correlated with tinnitus reduction (r=0.87). To avoid extremity in the correlation analysis, the patient with the maximum tinnitus reduction was removed.
Left and Right Ear Responsiveness
Greater tinnitus reductions were identified in left ears [Figure 1, A and B; Table 4 (p <0.05)]. This may be a result of cortical fibers from the left ear relaying information faster or more to the right brain than the left [16]. Additionally, the right hemisphere is more suited to processing longer auditory stimuli [17-19] and the suppressive noise spectrum is a long stimulus.
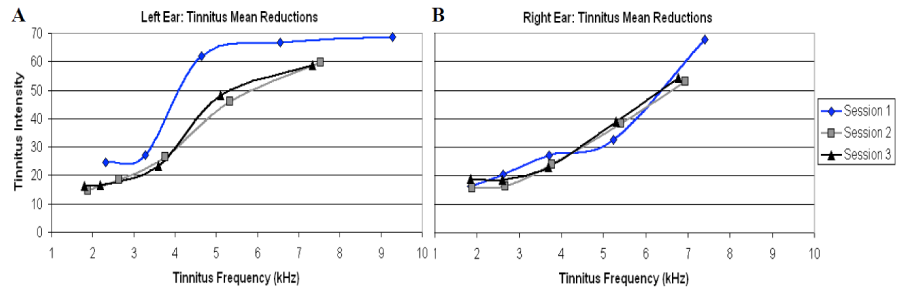
Figure 1: The mean changes in tinnitus intensity and frequency over sessions 1 to 3 across all patients. Visual representation of the mean changes in tinnitus intensity and frequency over sessions 1 to 3 across all patients in right ear tinnitus (A) and in left ear (B). Every of the three curves has 5 data points. Two data points at the left sides represent the suppressive frequencies near lower octave and half octave, while two data points at the right sides represent the suppressive frequencies near higher octave and half octave. The one in the middle between two left and two right sides is the tinnitus frequencies.
Listening Period
Listening 2 hours per day over 50 days appeared to be a needed duration, although patients who listened less than this (e.g., 80 hours over 50 days), still experienced improvement.
Limitations
Like other reports, this report also has limitations, especially as a first report on the novel suppressive spectrum. Distribution of our findings will promote further research in this area.
Our sample size was relatively small, but statistical significance still existed in key and multiple data analyses. Even in those analyses with p > 0.05, most data show a strong trend, which may become significant in future research.
Three months of therapy is relatively short. A longer duration may lead to increased improvement. Some patients listened less than 2 hours a day, yet significant results were still found (although listening <2 hours yields less improvement). This may be further improved in future research so that better results may be achieved.
Tinnitus is highly variable, increasing the likelihood of inconsistent outcomes. Some patients had concurrent disorders, increased hearing loss, or other factors (e.g., smoking), which may have negatively impacted improvement. A number of our patients had high frequency tinnitus, which may have affected our results, as research has found notched music therapy to be less effective for those experiencing this type [8].
CONCLUSIONS
Using suppression in tinnitus is novel. Based on our findings, using a customized suppressive noise spectrum is effective in shifting the frequency, reducing the intensity of subjective tonal tinnitus, and improving the handicap based on THQ test. From this seminal report, factors related to maximizing its effectiveness (e.g., length of listening time, level of hearing loss, and application for alternative tinnitus types) may be considerations for future research.
ACKNOWLEDGEMENT
The authors thank Dr. Ada Leung for her critical review and valuable comments on this project as well as her edit on the early version of this report. The project was partly supported by the institutional research grant for the project “Remapping tinnitus cortex” (MZ), Natural Sciences and Engineering Research Council of Canada (MZ), the Canada Foundation for Innovation (MZ), Canadian Institutes of Health Research (AJ), and the Glenrose Rehabilitation Hospital Foundation (MZ).
REFERENCES
- Baguley D, McFerran D, Hall D. Tinnitus. Lancet. 2013; 382: 1600-1607. Ref.: https://goo.gl/GZFggQ
- Heller AJ. Classification and epidemiology of tinnitus. Otolaryngol Clin North Am. 2003; 36: 239-248. Ref.: https://goo.gl/wvoR1H
- Langguth B, Kreuzer PM, Kleinjung T, De Ridder D. Tinnitus: Causes and clinical management. Lancet Neurol. 2013; 12: 920-930. Ref.: https://goo.gl/Qq5FHd
- Pape J, Paraskevopoulos E, Bruchmann M, Wollbrink A, Rudack C, et al. Playing and listening to tailor-made notched music: Cortical plasticity induced by unimodal and multimodal training in tinnitus patients. Neural Plast.2014;2014: 1-10. Ref.: https://goo.gl/ZUnKcF
- Jackson JG, Coyne IJ, Clough PJ. A preliminary investigation of potential cognitive performance decrements in non-help-seeking tinnitus sufferers. Int J Audiol.2014; 53: 88-93. Ref.: https://goo.gl/ezcBJF
- Mohamad N, Hoare DJ, Hall DA. The consequences of tinnitus and tinnitus severity on cognition: A review of the behavioral evidence. Hear Res.2015; 1-11. Ref.: https://goo.gl/15XEXu
- Erlandsson SI, Hallberg LR. Prediction of quality of life in patients with tinnitus. Brit J Audiol. 2000; 34: 11-20. Ref.: https://goo.gl/fY7rtj
- Pantev C, Rudack C, Stein A, Wunderlich R, Engell A, et al. Study protocol: Münster tinnitus randomized controlled clinical trial-2013 based on tailor-made notched music training (TMNMT). BMC Neurol. 2014; 14: 14-40. Ref.: https://goo.gl/sM5wTQ
- Stracke H, Okamoto H, Pantev C. Customized notched music training reduces tinnitus loudness. Commun Integr Biol. 2010; 3: 274-277. Ref.: https://goo.gl/eSJLM5
- Teismann H, Okamoto H, Pantev C. Short and intense tailor-made notched music training against tinnitus: The tinnitus frequency matters. PLOS ONE. 2011; 6. Ref.: https://goo.gl/zD1747
- Okamoto H, Stracke H, Stoll W, Pantev C. Listening to tailor-made notched music reduces tinnitus loudness and tinnitus-related auditory cortex activity. Proc Natl Acad Sci U S A. 2010; 107: 1207-1210. Ref.: https://goo.gl/hgAQFN
- Ariizumi Y, Hatanaka A, Kitamura K. Clinical prognostic factors for tinnitus retraining therapy with a sound generator in tinnitus patients. J Med Dent Sci.2010; 57: 45-53. Ref.: https://goo.gl/YcqVbV
- Hobson J, Chisholm E, El Refaie A. Sound therapy (masking) in the management of tinnitus in adults. Cochrane Database Syst Rev. 2012; 11: 1-25. Ref.: https://goo.gl/FLq6gj
- Meeus O, Heyndrickx K, Lambrechts P, De Ridder D, Van de Heyning P. Phase-shift treatment for Tinnitus of cochlear origin. Eur Arch Otorhinolaryngol. 2010; 267: 881-888. Ref.: https://goo.gl/LjXaoN
- De Ridder D, Vanneste S, Weisz N, Londero A, Schlee W, et al. An integrative model of auditory phantom perception: Tinnitus as a unified percept of interacting separable subnetworks. Neurosci Biobehav Rev. 2013;44: 16-32. Ref.: https://goo.gl/a9aEmY
- Majkowski J, Bochenek Z, Bochenek W, Knapik-Fijałkowska D, Kopeć J. Latency of averaged evoked potentials to contralateral and ipsilateral auditory stimulation in normal subjects. Brain Res. 1971; 25: 416-419. Ref.: https://goo.gl/UdDRKv
- Poeppel D. The analysis of speech in different temporal interaction windows: Cerebral lateralization as ‘asymmetric sampling in time’. Speech Commun. 2003; 41: 245-255. Ref.: https://goo.gl/ARjYMm
- Zatorre RJ, Belin P, Penhune VB. Structure and function of auditory cortex: Music and speech. Trends Cogn Sci. 2002; 6: 37-46. Ref.: https://goo.gl/PueT7K
- Zatorre RJ, Grandour JT. Neural specializations for speech and pitch: Moving beyond the dichotomies. Philos Trans R Soc Lond B Biol Sci. 2008; 363: 1087-1104. Ref.: https://goo.gl/3kKH2s