
More Information
Submitted: January 12, 2026 | Accepted: January 21, 2026 | Published: January 22, 2026
Citation: Cao Q, Kang C, Gu K, Peng Y, Lv Y, Ding XZ, et al. Transumbilical Single-incision Hiatal Hernia Repair and Nissen Fundoplication in situs Inversus Totalis: A Rare Case Report. Adv Treat ENT Disord. 2026; 10(1): 001-003. Available from:
https://dx.doi.org/10.29328/journal.ated.1001017.
DOI: 10.29328/journal.ated.1001017
Copyright license: © 2026 Cao Q, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Situs inversus totalis; Hiatal hernia; Gastroesophageal Reflux Disease (GERD); Laparoscopic surgery; Single-Incision Surgery (SILS); Nissen fundoplication; Gastrointestinal surgery; Hernia repair; Gastrogram; Endoscopy; CT scan

Transumbilical Single-incision Hiatal Hernia Repair and Nissen Fundoplication in situs Inversus Totalis: A Rare Case Report
Qing Cao, Chen Kang, Kang Gu, Yin Peng, Yang Lv, Xu-Zhong Ding and Peng Li*
Department of Gastroenterology, The Affiliated Hospital of Nantong University, Jiangsu Province, China
*Corresponding author: Peng Li, Department of Gastroenterology, The Affiliated Hospital of Nantong University, Jiangsu Province, China, Email: [email protected]
In this manuscript, we present an Hiatal hernia(HH) with situs inversus totalis(SIT) performed by transumbilical single-incision laparoscopic hiatal hernia repair and Nissen fundoplication, which is rarely reported previously. A 62-year-old woman was admitted with a diagnosis of hiatal hernia and gastroesophageal reflux disease (GERD), as proven by Gastroesophageal Reflux Disease Questionnaire (GERD-Q) scoring, endoscopic, and radiologic findings. The patient had a history of spinal correction surgery for scoliosis five years ago, during which her SIT was identified. We performed a classic LHHR plus Nissen fundoplication for the patient, especially through a transumbilical single incision. An atraumatic method of liver retraction with a Veress needle sheathed by a latex tube and a convenient autosuturing device was used to overcome the difficulties. The patient experienced an uneventful recovery and presented complete resolution of GERD at the one-month follow-up.
Hiatal hernia (HH) is an anatomical defect through which the stomach or other intra-abdominal organs protrude into the thoracic cavity. It can cause displacement of the esophageal-gastric junction into the thorax and disruption of the anti-reflux barrier, leading to gastroesophageal reflux disease (GERD). Though GERD-related symptoms can be alleviated by antacid usage, laparoscopic hiatal hernial repair (LHHR) plus fundoplication has been recognized as an effective treatment for HH when medical therapy fails.
Situs Inversus Totalis (SIT) is a genetic anomaly characterized by the arrangement of the abdominal and thoracic organs in a perfect mirror image reversal of the normal positioning. Transposition of the organs poses challenges for operators who are used to the routine anatomy.
In this manuscript, we present an HH case with SIT performed by transumbilical single-incision LHHR and Nissen fundoplication, which is rarely reported previously.
A 62-year-old woman was admitted with a five-decade history of classic gastroesophageal reflux symptoms, including heartburn, chest pain, and postprandial regurgitation. The Gastroesophageal Reflux Disease Questionnaire (GERD-Q) yielded a score of 6 points. The long -term damage caused by reflux was further confirmed by endoscopy, with a shift of the EGJ to 33 cm from the incisors and erosion of the esophageal mucosa (Figure 1).
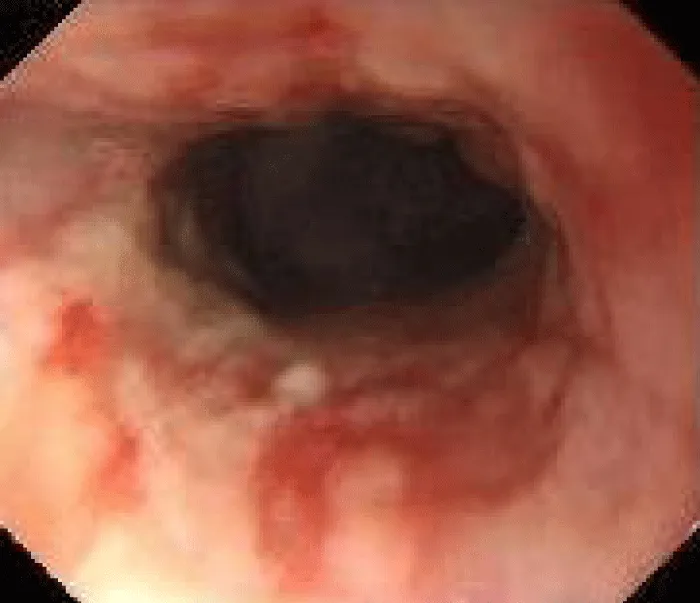
Figure 1: Endoscopic view.
The patient had a history of spinal correction surgery for scoliosis five years ago, during which her SIT was identified. Our CT exam and gastrogram proved her history, with a hernia sac measuring 35*48 mm (Figures 2-4). All routine laboratory tests were within normal limits.

Figure 2: Front view of the gastrogram before surgery.
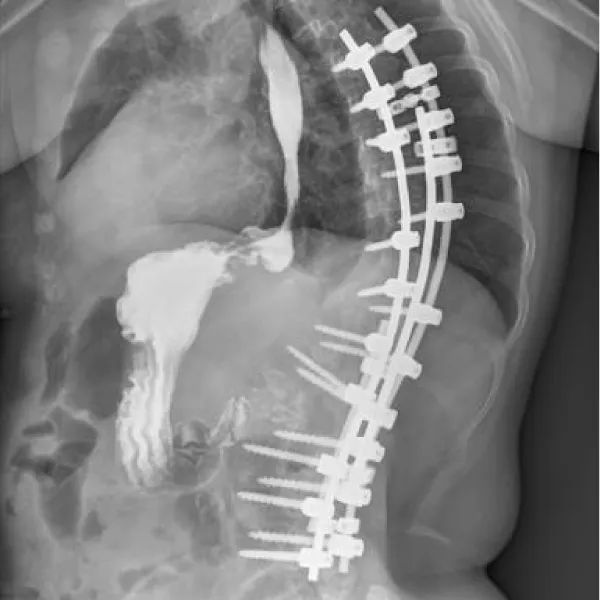
Figure 3: Lateral view of the gastrogram before surgery.
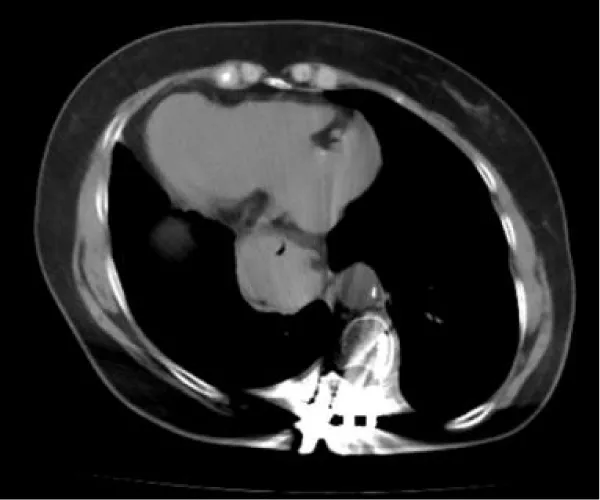
Figure 4: Abdominal CT before surgery.
Considering the refractory GERD-related symptoms attributed to HH, we performed a classic LHHR plus Nissen fundoplication for the patient, especially through a transumbilical single incision.
The patient was prepared in a supine position, with the operating surgeon standing on the right side of the patient and the scope holder on the left. A 3-cm horizontal incision was made at the umbilicus, followed by the insertion of a single-port platform and the establishment of pneumoperitoneum. To expose the peri-hiatal area, a Veress needle was inserted below the right costal margin, followed by insertion of a latex tube to atraumatically retract the liver (Figure 5). Intraoperative exploration confirmed the presence of SIT within the abdominal cavity and type I HH. The diameter of the hiatal defect expanded to approximately 3 cm. After standardized dissection, the defect was repaired by firstly approximating the crura with a running 3-0 barbed suture and then reinforcement with a 3-0 nonabsorbable suture applied with an autosuturing device (Figure 6). Nissen fundoplication was completed in a counterclockwise fashion with approximation and reinforcement in the same way (Figure 7). During the wrapping maneuver, a 36F bougie was inserted through the gastric cardia to ensure the appropriate tightness. Finally, no drainage was placed, and the umbilical incision was properly closed. Postoperative recovery was uneventful. The patient took a liquid diet on the first day after surgery and was discharged three days later. At the interview in one month, she was free of GERD-related symptoms or dysphagia, and scored 0 points in GERD-Q. The follow-up CT and gastrogram were consistent with the presentation, indicating complete resolution of GERD (Figures 8,9).
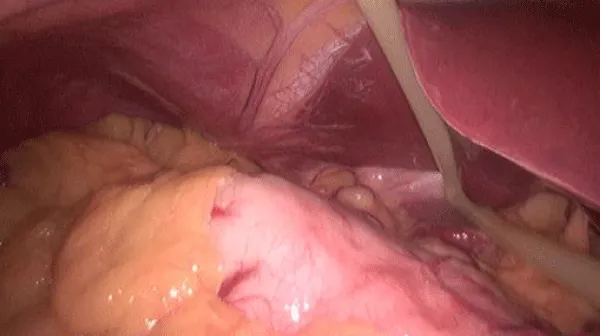
Figure 5: Liver retraction with a self-made device..
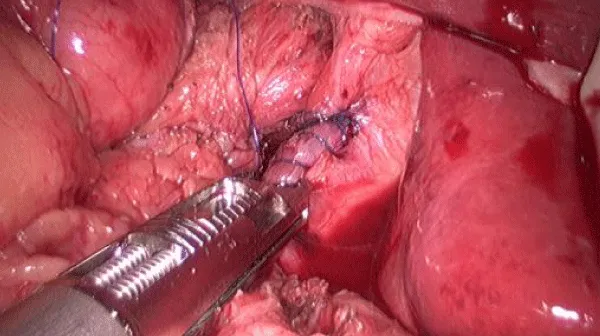
Figure 6: Approximation of the crura with an auto-suturing device.
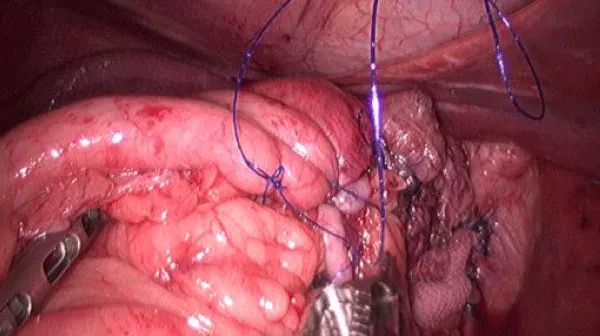
Figure 7: Fundoplication counterclockwise.

Figure 8: Front view of the gastrogram one month after surgery.

Figure 9: Abdominal CT one month after surgery.
Situs inversus totalis is defined by a complete reversal of the positions of thoracic and abdominal viscera to the contralateral sides of the body. As a rare autosomal recessive condition, it affects approximately 0.003% of the population [1]. Though situs anomaly is associated with gastrointestinal abnormalities, including hiatal hernia, SIT, as a mirror image of the normal anatomy, seems to have no impact on health. However, it does elicit confusion in intra-operative communication and performing fundoplication in the opposite direction [1]. SIT didn’t interfere with the positions of the surgeon and the scope holder, as we employed in previous operations with normal anatomy.
Another risk factor for our patient is the history of scoliosis. In a previous study, spinal deformity was present in 15.8% of the patients undergoing hiatal hernia repair, with scoliosis accounting for 58.6%. This group of patients displayed more complex hernia types, larger hernia sizes, higher recurrence rates, and shorter time to recurrence [2]. It is speculated that abnormal spinal curvature decreases the tensile strength of the diaphragm by affecting its structure. This alteration can also be found in the film of our patient, with a flattened and elongated diaphragm. Fortunately, our patient had had her spinal deformity corrected, which avoided the use of a mesh and lowered the risk of complications.
Transumbilical single-incision laparoscopic surgery (SILS), as an innovative technique, has been expanding its indications in recent years. Advantages such as better cosmetic outcomes, reduced postoperative pain, and faster recovery period are further amplified than those of traditional minimally invasive surgeries. In spite of this, application in hiatal herniorraphy is scarcely reported. Besides the common problem of instrument conflicts, which can be solved by extended instruments, the hiatal herniorrhaphy features special considerations. Firstly, adequate retraction of the liver is crucial for single-operator surgery. Some methods have been invented to overcome this obstacle, such as a traditional liver retractor, a stay suture, or glue adhesion [3]. We devised an innovative technique by inserting a Veress needle subcostally and sheathing it with a latex tube [4]. We prefer this method not only for its flexibility and scarless entrance, but also for the effectiveness of the extended part of the tube beyond the needle tip to push away the omentum. Secondly, one-hand suturing of the diaphragmatic crura is inevitable when the left hand of the surgeon has to elevate the esophagus. We overcame the difficulty of interhand cooperation in pulling and knotting by applying an autosuturing device equipped with a nonabsorbable barbed suture.
The uneventful recovery and alleviation of the symptoms at 1-month follow-up supported the safety and efficacy of the surgery. It is a successful attempt at transumbilical single-incision surgery in hiatal herniorrhaphy, though some techniques in manipulation and visualization are still to be improved. With more experience and evidence, we hope to explore the possibility for patients with indications of mesh implant.
Ethical approval: I declare on my honor that the ethical approval has been exempted by my establishment.
- Haran C, Fischer N, Oliver T, Grant M. Mirror-image confusion: successful giant hiatus hernia repair in situs inversus totalis. N Z Med J. 2019;132(1496):66-68. Available from: https://pubmed.ncbi.nlm.nih.gov/31170135/
- Perisetla N, Doyle WN Jr, Ladehoff L, Natarelli N, Nemov V, Pittala K, et al. Effects of Spinal Deformities on Hiatal Hernia Occurrence and Recurrence. J Gastrointest Surg. 2023;27(12):2718-2723. Available from: https://doi.org/10.1007/s11605-023-05877-5
- Hamzaoglu I, Karahasanoglu T, Aytac E, Karatas A, Baca B. Transumbilical totally laparoscopic single-port Nissen fundoplication: a new method of liver retraction: the Istanbul technique. J Gastrointest Surg. 2010;14(6):1035-9. Available from: https://doi.org/10.1007/s11605-010-1183-1
- Yu X, Cao Q, Feng Y, Li M, Li P. Application of a modified liver retraction technique for laparoscopic bariatric surgery. Chinese Journal of Obesity and Metabolic Diseases (Electronic Edition). 2023;9(4):246–252. Available from: https://zhfpydxbdzzz.cma-cmc.com.cn/CN/10.3877/cma.j.issn.2095-9605.2023.04.004