
More Information
Submitted: 17 May 2023 | Approved: 30 May 2023 | Published: 31 May 2023
How to cite this article: Armone Caruso A, Miglietta A, De Rossi G, Nappi L, Viola V, et al. Nasal cytology in patients with previous SARS-CoV-2 infection: occurrence of atypical lymphocytes. Adv Treat ENT Disord. 2023; 7: 001-006.
DOI: 10.29328/journal.ated.1001014
Copyright License: © 2023 Armone Caruso A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Nasal cytology; SARS-CoV-2; Atypical lymphocytes; Rhinitis; Viral rhinitis; Rhino-fibroscopy

Nasal cytology in patients with previous SARS-CoV-2 infection: occurrence of atypical lymphocytes
Arturo Armone Caruso1*, Anna Miglietta2, Giovanni De Rossi3, Liliana Nappi4, Veronica Viola5, Stefano De Rossi2, Salvatore Del Prete6, Clara Imperatore7, Sabato Leo8, Daniele Naviglio9, Monica Gallo10, Daniela Marasco6 and Lucia Grumetto11
1Health Director and Department of Otolaryngology, AIAS, Afragola, 80021 Naples, Italy
2ENT Outpatient Clinic at Legnago Mater Salutis Hospital, Legnago (Verona) Italy
3Outpatient Specialist in ENT, Studi Santa Chiara, Verona, Italy
4Outpatient Specialist in Allergology and Clinical Immunology, Scafati, Salerno, Italy
5Department of Engineering, University of Campania “Luigi Vanvitelli” II, via Roma, 29, 81031 Aversa, Italy
6Service Biotech srl, Via Monte di Dio 80, Naples, 80132, Italy
7Outpatient Specialist in Allergology and Clinical Immunology ASL Napoli 1 Centro, UO, Naples, Italy
8ENT Outpatient Clinic at Scafati Hospital ASL SA, 84018 Salerno, Italy
9Department of Chemical Sciences, University of Naples Federico II, Naples 80126, Italy
10Department of Molecular Medicine and Medical Biotechnology, University of Naples Federico II, via Pansini, 5, 80131 Naples, Italy
11Department of Pharmacy, University of Naples Federico II, Via Montesano 49, 80131 Naples, Italy
*Address for Correspondence: Arturo Armone Caruso, Health Director and Department of Otolaryngology, AIAS, Afragola, 80021 Naples, Italy, Email: [email protected]
SARS-CoV-2 is a new pandemic infection that affects at the beginning the upper respiratory system, and, successively, all the organisms, due to cytokine storm, with serious consequences that can reach death. The aim of this work was the observation of the nasal mucosa of enrolled 60 patients, resulting negative for two weeks to the molecular swab for SARS-CoV-2, versus the control group. Rhino-fibroscopy and nasal cytology of nasal mucosa were performed for both the investigated groups. The observation of the samples showed the occurrence of plasmablastic lymphocytes and Downey II lymphocytes type. The former type of lymphocytes was prevalent against the second one, probably because of an immunological “scar”. The rhino-fibroscopy showed a “pseudo ischemia of nasal submucosa” at pre and pericranial levels, not occurred in the control group.
The occurrence of atypical lymphocytes in the nasal smear was analog to that observed in the blood peripheral smear, probably caused by mechanisms of local immune reaction and dysregulation like those observed in other virus infections. Our findings suggest that the nasal mucosa study through the nasal cytology, can represent an important predictive tool of the SARS-CoV-2 infection.
SARS-CoV-2 is an RNA virus of the Beta coronavirus family [1], that affects the upper respiratory tract. According to Sungnak, et al. [2], in this severe acute respiratory syndrome, both the genes involved in innate immunity highly co-expressed in nasal epithelial cells and endogenous factors highlighted the crucial role of the nose at the beginning of a viral transmission to all the organisms [3]. Nevertheless, the infection can occur with weak symptoms, i.e. nasal edema and/or rhinorrhea, despite other viral rhinitis (i.e., adenovirus, rhinovirus influenza, etc.), featured by more relevant typical nasal symptoms such as sneezings, rhinorrhoea and nasal edema [4]. This virus shares genomic and clinical similarities with other highly pathogenic coronaviruses, (SARS-CoV, MERS-CoV), which caused deadly outbreaks in 2002 and 2012 respectively. SARS-CoV-2 infection can range from asymptomatic to respiratory symptoms mild to fatal acute respiratory distress syndrome.
Usually, cell infiltration begins on the first day of the infection, and neutrophils, lymphocytes, and exfoliated epithelial cells characterize the cytopathological feature [5]. A typical sign of cell injury is the “Ciliocytophthoria”, featured by condensed nuclear chromatin, marginalization of nucleoli, inclusion bodies, perinuclear halo, and cytoplasmic vacuoles [6]. Furthermore, typical evidence of the anatomical and functional integrity of the ciliated cells, is the occurrence of the “hyperchromatic supranuclear stria” (SNS), as an indicator of Golgi activity [7]; the latter disappearance during viral infection indicates cell distress [8]. The ciliated cells seem to be the first target of the virus replication SARS-CoV-2, along with the presence of pathological epithelial cells like other viral infections [9,10].
Moreover, several pieces of evidence are still quite unclear, and they could represent a further element of study and diagnosis, such as the study of nasal lymphocytes in subjects affected by SARS-CoV-2, to prevent and monitor the illness. The scope of this research work is the characterization of the lymphocytes of nasal mucosa in infected SARS-CoV-2 patients versus a control group.
To perform this clinical research, 60 patients were enrolled (30 males and 30 females, age range 30-60 years, average 45.6), by our Department of “AIAS” (Associazione Italiana Assistenza Svantaggiati) of Afragola, Naples, Italy. The Ethics Committee of the coordinating center AIAS approved the study protocol. All patients were required of written informed consent, before study inclusion. Before the study began, all subjects have been subjected to a molecular swab test as an assurance of negative SARS- CoV-2.
All patients admitted to the study resulted not affected by other diseases and they were not in drug therapy, on the other hand, they showed a persistence of nasal obstruction and hyposmia of varying degrees, weak respiration, and, therefore, they were in rehabilitation treatment.
As a control group, patients, non-smokers, not subjected to any therapy neither pharmacological nor rehabilitative, not affected by other infections, and without diseases, were recruited.
For each patient, cytological sampling from each naris was carried out using the scraping technique with a probe (Nasal-scraping®), performing 2-3 smears on the mucous surface of the middle third of the inferior turbinate.
The sample, placed on an electrostatically charged cytology slide (Superfrost Plus Menzel-Gläser, Thermo Scientific, Milan, Italy,) was stained according to the panoptic method i.e.: 3 min pure May-Grunwald dye (Carlo Erba, Milan, Italy), 6 min in 50% May-Grunwald dye, 1 minute in distilled water (Carlo Erba, Milan, Italy) and finally 30 minutes in diluted 1:10 v/v Giemsa solution (Carlo Erba, Milan, Italy).
The slides, covered with a coverslip measuring 24 × 60 mm #1, were observed with an optical microscope (Nikon Eclipse 50i), with immersion magnification of 1000 ×; a semi-quantitative evaluation was conducted on fifty observational fields, as indicated by the AICNA (Italian Academy of Nasal Cytology) [11]. The images were recorded using a Nikon DS1 camera and digitized using NIS-D Elements.
Finally, a rhino-fibroscopy was performed with 0° and 30° rigid optics with a diameter of 2.7 mm and length of 11 cm, recorded using a device Storz image 1 full HD camera plus S.P.I.E.S. (Storz Professional Image Enhancement System), connected to an informatic database. Observation and recording were performed in standard mode, clara + chroma in order to show intramucosal vascularization and also in spectra B mode, to highlight superficial vascularization (intra and submucosal). The control group was undergoing to the same evaluation procedure. Images and slide observation were performed by both the study groups, i.e. Naples and Verone (Italy), to be aware of subjective observations.
All the subjects recovered by SARS-CoV-2 infection showed atypical and activated lymphocytes, for their features, beyond that cell alterations such as polinucleations and distinctive Ciliocitophtoria (Figure 1). Two types of lymphocytes with different characteristics were highlighted by the cytology observation: a) Plasmacytoid (Figure 2), small mature lymphocytes with an eccentric nucleus and dark blue cytoplasm; this category includes cells with plasmablastic characteristics in which the nucleus is slightly larger with open chromatin and a prominent nucleolus; b) Downey II-like cells (Figure 3): large lymphocytes, and rare cytoplasmic granules, similar, as morphology, to the original Downey II cells. Moreover, we observed a higher percentage of atypical Plasmacytoid lymphocytes than Downey II. The summary of our findings is reported in Table 1. The rhino-fibroscopy technique showed a “psuedoischemia submucosa” in 62% of previously affected by SARS-CoV-2 subjects under our investigation, mostly in the posterior area (Figure 4). Moreover, there is evidence of a significant increase in the vascular submucosa in about 89% of the investigated subjects (Figure 5). These findings were not founded in the subjects of the control group.
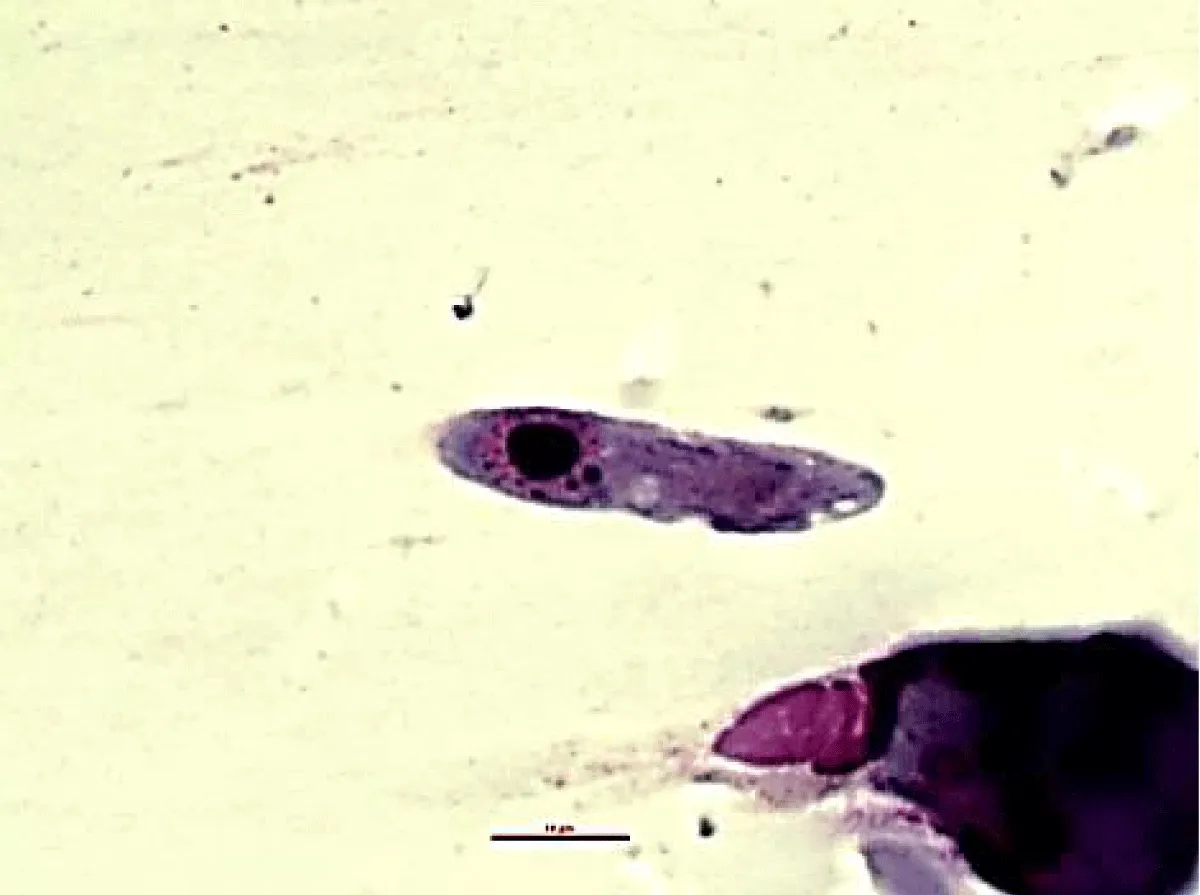
Figure 1: “Ciliocytophthoria". Observation by optical microscope. Magnification at 1000 X oil immersion. Col. MGG.
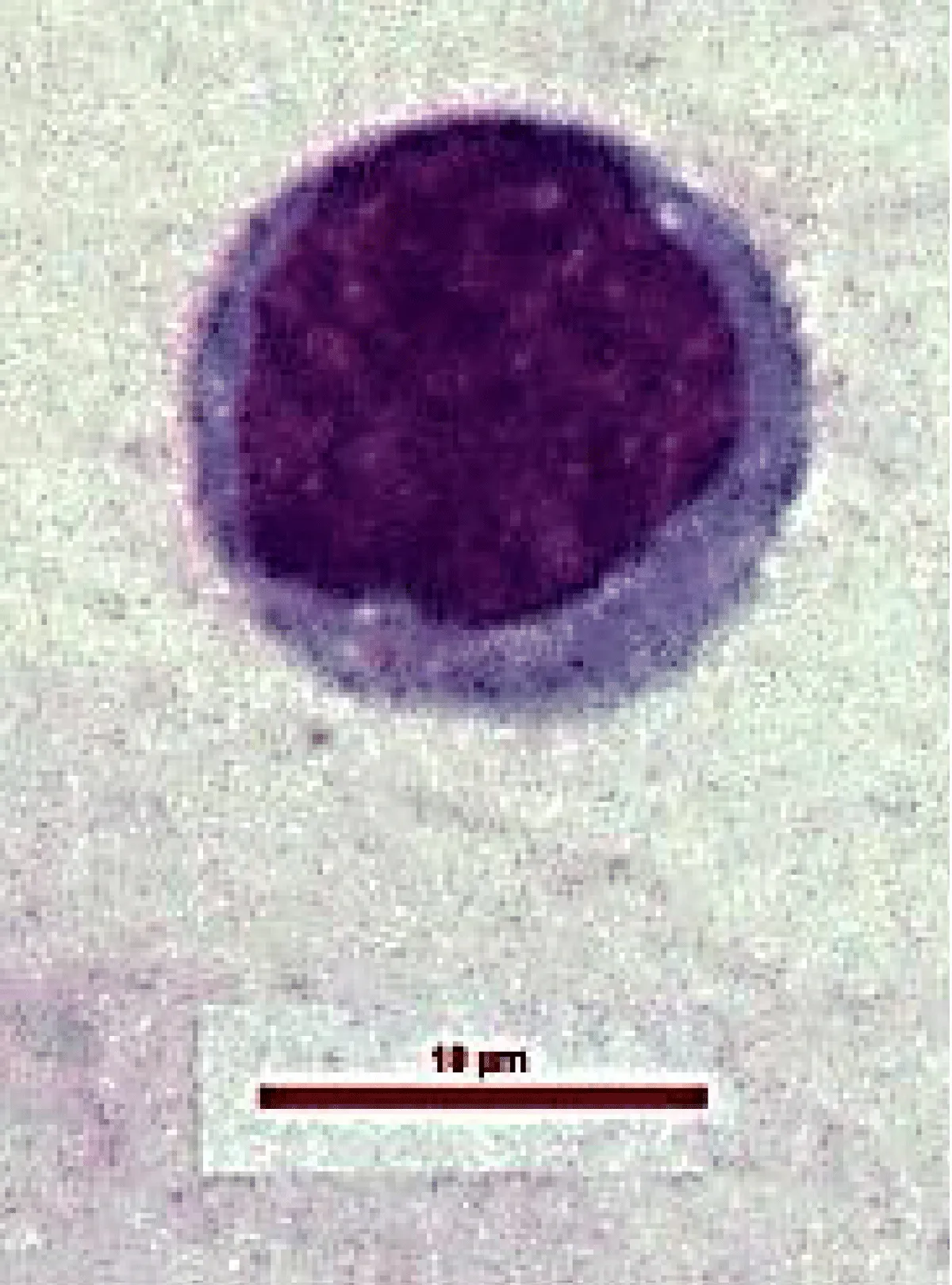
Figure 2: Atypical lymphocytes showing plasmacytoid features including small size, eccentric nucleus and dark blue cytoplasm.
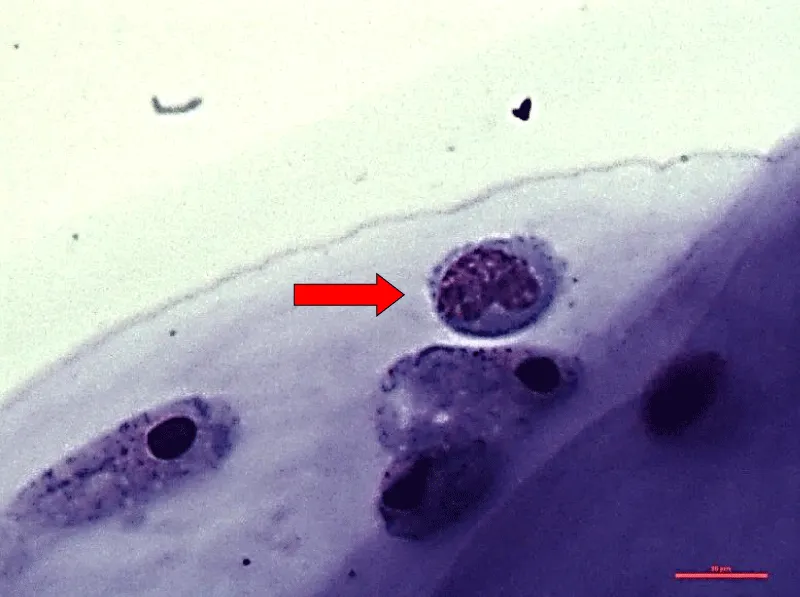
Figure 3: Atypical lymphocytes with Downey II-like (red arrow) cells features showing large size, ample cytoplasm, indented nucleus, and occasional cytoplasmic granules. Magnification at 1000 x oil immersion. Col. MGG.
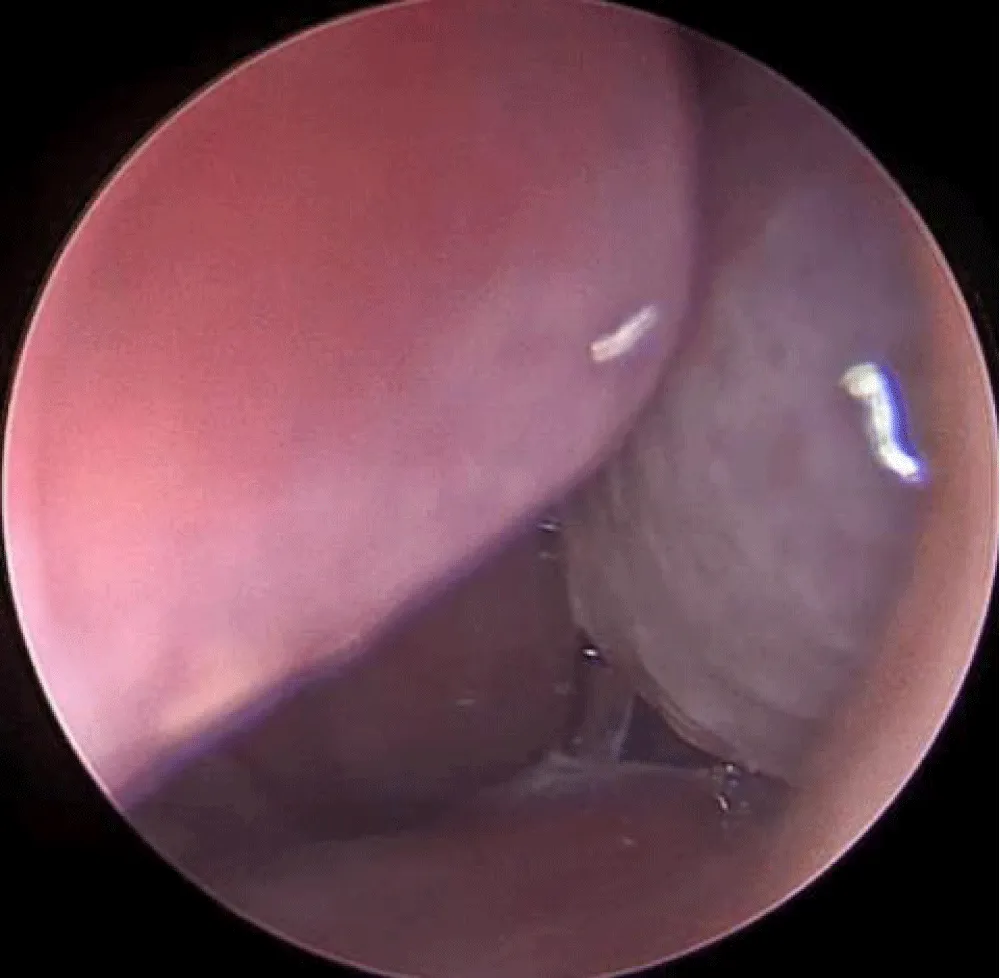
Figure 4: Observation performed with a rigid 0° rhinofibroscope. In posterior region of the turbinate lower submucosal psueudoischemia.
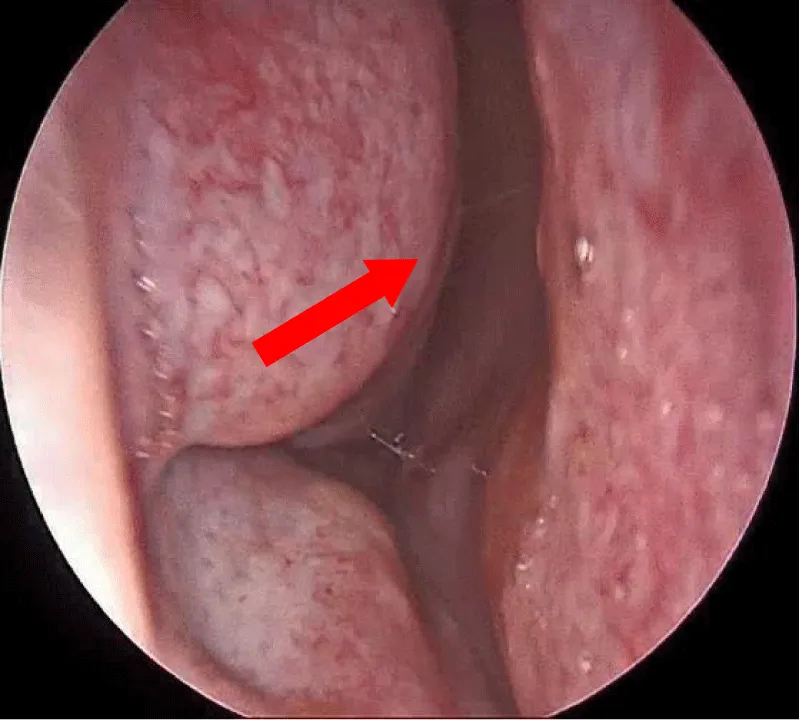
Figure 5: Observation performed with a rigid 0° rhinofibroscope. Significant increase of the vascular submucos (red Arrow).
| Table 1: Summary of SARS-CoV-2 patients and control group. | |||||||||||
| SARS-CoV-2 Patients | Age | Gender | N* Plasmocitoid cells |
N* Downey II cells |
N* Normal morphology cells |
Control group patiens | Age | Gender | N* Plasmocitoid cells |
N* Downey II cells |
N* Normal morphology cells |
| 1 | 30 | M | 20 | 10 | 1 | 1 | 30 | M | 0 | 0 | 1 |
| 2 | 35 | M | 15 | 7 | 2 | 2 | 35 | M | 0 | 0 | 2 |
| 3 | 30 | F | 24 | 12 | 5 | 3 | 30 | F | 0 | 0 | 0 |
| 4 | 38 | M | 12 | 4 | 6 | 4 | 38 | M | 0 | 0 | 0 |
| 5 | 36 | M | 6 | 1 | 2 | 5 | 36 | M | 0 | 0 | 1 |
| 6 | 37 | F | 10 | 2 | 5 | 6 | 37 | F | 0 | 0 | 1 |
| 7 | 38 | M | 43 | 21 | 1 | 7 | 38 | M | 0 | 0 | 1 |
| 8 | 40 | F | 25 | 15 | 1 | 8 | 40 | F | 0 | 0 | 1 |
| 9 | 43 | M | 34 | 21 | 1 | 9 | 43 | M | 0 | 0 | 0 |
| 10 | 44 | F | 23 | 12 | 0 | 10 | 44 | F | 0 | 0 | 0 |
| 11 | 60 | M | 15 | 8 | 0 | 11 | 60 | M | 0 | 0 | 0 |
| 12 | 55 | F | 10 | 3 | 0 | 12 | 55 | F | 0 | 0 | 0 |
| 13 | 60 | F | 32 | 25 | 0 | 13 | 60 | F | 0 | 0 | 2 |
| 14 | 59 | F | 28 | 14 | 1 | 14 | 59 | F | 0 | 0 | 5 |
| 15 | 55 | M | 35 | 12 | 1 | 15 | 55 | M | 0 | 0 | 1 |
| 16 | 59 | F | 23 | 12 | 0 | 16 | 59 | F | 0 | 0 | 2 |
| 17 | 44 | M | 12 | 6 | 0 | 17 | 44 | M | 0 | 0 | 1 |
| 18 | 48 | M | 10 | 1 | 0 | 18 | 48 | M | 0 | 0 | 0 |
| 19 | 45 | F | 13 | 0 | 0 | 19 | 45 | F | 0 | 0 | 2 |
| 20 | 37 | F | 22 | 8 | 0 | 20 | 37 | F | 0 | 0 | 0 |
| 21 | 40 | M | 54 | 12 | 0 | 21 | 40 | M | 0 | 0 | 0 |
| 22 | 33 | F | 56 | 11 | 0 | 22 | 33 | F | 0 | 0 | 0 |
| 23 | 36 | F | 23 | 12 | 0 | 23 | 36 | F | 0 | 0 | 0 |
| 24 | 39 | F | 21 | 13 | 0 | 24 | 39 | F | 0 | 0 | 0 |
| 25 | 40 | F | 23 | 11 | 0 | 25 | 40 | F | 0 | 0 | 1 |
| 26 | 37 | F | 24 | 12 | 0 | 26 | 37 | F | 0 | 0 | 5 |
| 27 | 38 | M | 18 | 7 | 0 | 27 | 38 | M | 0 | 0 | 0 |
| 28 | 44 | F | 19 | 6 | 0 | 28 | 44 | F | 0 | 0 | 4 |
| 29 | 45 | M | 25 | 9 | 0 | 29 | 45 | M | 0 | 0 | 0 |
| 30 | 54 | F | 15 | 8 | 0 | 30 | 54 | F | 0 | 0 | 0 |
| 31 | 54 | M | 23 | 12 | 0 | 31 | 54 | M | 0 | 0 | 0 |
| 32 | 60 | F | 33 | 10 | 0 | 32 | 60 | F | 0 | 0 | 0 |
| 33 | 58 | M | 44 | 12 | 0 | 33 | 58 | M | 0 | 0 | 0 |
| 34 | 39 | F | 55 | 23 | 0 | 34 | 39 | F | 0 | 0 | 0 |
| 35 | 44 | F | 43 | 34 | 1 | 35 | 44 | F | 0 | 0 | 5 |
| 36 | 44 | M | 32 | 25 | 0 | 36 | 44 | M | 0 | 0 | 0 |
| 37 | 39 | M | 23 | 12 | 1 | 37 | 39 | M | 0 | 0 | 0 |
| 38 | 41 | F | 34 | 24 | 1 | 38 | 41 | F | 0 | 0 | 8 |
| 39 | 39 | M | 45 | 23 | 1 | 39 | 39 | M | 0 | 0 | 0 |
| 40 | 37 | F | 52 | 25 | 0 | 40 | 37 | F | 0 | 0 | 0 |
| 41 | 39 | F | 32 | 12 | 0 | 41 | 39 | F | 0 | 0 | 0 |
| 42 | 36 | M | 12 | 7 | 0 | 42 | 36 | M | 0 | 0 | 3 |
| 43 | 45 | M | 32 | 13 | 0 | 43 | 45 | M | 0 | 0 | 0 |
| 44 | 42 | F | 21 | 12 | 0 | 44 | 42 | F | 0 | 0 | 0 |
| 45 | 43 | M | 55 | 44 | 0 | 45 | 43 | M | 0 | 0 | 5 |
| 46 | 57 | M | 55 | 32 | 0 | 46 | 57 | M | 0 | 0 | 0 |
| 47 | 53 | M | 34 | 23 | 0 | 47 | 53 | M | 0 | 0 | 0 |
| 48 | 52 | F | 12 | 14 | 0 | 48 | 52 | F | 0 | 0 | 0 |
| 49 | 57 | M | 33 | 12 | 1 | 49 | 57 | M | 0 | 0 | 5 |
| 50 | 53 | F | 31 | 14 | 1 | 50 | 53 | F | 0 | 0 | 0 |
| 51 | 54 | M | 32 | 18 | 0 | 51 | 54 | M | 0 | 0 | 0 |
| 52 | 57 | M | 33 | 15 | 0 | 52 | 57 | M | 0 | 0 | 0 |
| 53 | 56 | F | 44 | 15 | 0 | 53 | 56 | F | 0 | 0 | 2 |
| 54 | 38 | F | 53 | 22 | 0 | 54 | 38 | F | 0 | 0 | 0 |
| 55 | 34 | M | 32 | 22 | 0 | 55 | 34 | M | 0 | 0 | 0 |
| 56 | 54 | M | 44 | 12 | 0 | 56 | 54 | M | 0 | 0 | 0 |
| 57 | 52 | F | 21 | 16 | 0 | 57 | 52 | F | 0 | 0 | 0 |
| 58 | 50 | M | 12 | 7 | 0 | 58 | 50 | M | 0 | 0 | 2 |
| 59 | 54 | F | 23 | 12 | 0 | 59 | 54 | F | 0 | 0 | 0 |
| 60 | 56 | M | 12 | 9 | 0 | 60 | 56 | M | 0 | 0 | 2 |
| N*=number. | |||||||||||
The observation of the nasal mucosa shows the occurrence of atypical lymphocytes different in their features to those observed in the samples of the control group, but analogues to those identified in the peripheral blood smear [12-14] in patients previously affected by Coronavirus syndrome [15]. Laboratory results referred to leukopenia, lymphopenia, monocytosis, neutrophilia, eosinopenia, and thrombocytopenia, associated with COVID-19 infection [16-18]. The literature reports various scientific works concerning morphological results of atypical lymphocytes in peripherical blood smear [19,20], while to date there is no evidence of scientific reports that have observed atypical lymphocytes in nasal mucosa in SARS-CoV-2 patients. Our previous scientific work highlighted the occurrence of nasal lymphocytes against Epstein Barr virus [21] and other works describe the immunity reaction of the nasal mucosa [2,22,23].
The optical microscope observation shows the presence of atypical lymphocytes with two different cytological characteristics of inflammation, in all patients infected by SARS-CoV-2: a) Plasmacytoid-type lymphocytes; b) Atypical Downey II type lymphocytes, with the former prevailing respect to the Downey II type lymphocytes type, according to those reported by other authors on peripheral blood smear [9,24-27].
The evident occurrence of lymphocytes allows us to hypothesize that, through an immune dysfunction of the T lymphocytes, the virus can act through a mechanism of activation of the Nasal Associated Lymphoid Tissue, (NALT), the first “gate control”, for all immunocompetent mucous membranes. In consequence, the most severe onset of symptoms occurs especially in those patients with impaired local intrinsic immunity [2,26], which results in monocyte/macrophage activation, uncontrolled cytokine release, and fatal multiorgan dysfunction.
Although atypical lymphocyte morphology is rare in viral infections, viruses that cause pneumonia, such as influenza A, SARS-1, and swine flu, are not commonly associated with atypical lymphocyte morphology [28,29]. Other viral infections are associated with plasmacytoid lymphocytes, such as Dengue fever and, to a lesser extent in Rubella infection [30].
The results of this study show the presence of unique features of the SARS-CoV-2 infection, also in the nasal mucosa, that may be due to immune reaction mechanisms and local deregulation, uncommonly in other virus infections.
The ischemia of the nasal submucosa, could, therefore, be considered the local effect caused by the simultaneous action of the immune and/or inflammatory response and the viral disease, which, in turn, can lead to peripheral vascularity diffuse damage of upper airways [31]. Furthermore, the pseudoischemia could be caused by the enhanced action of proinflammatory cytokines, such as IL-6, Tnfa and IL-8 and caused by reduced type I and III interferons [32-40].
The nasal cytological study, proposed in this study on patients with a previous SARS-COV-2 infection, allowed us to identify lymphocyte features similar to those observed in peripheral blood smears of these patients as reported in the literature [11-15]. Our observations relate the occurrence of atypical lymphocytes to NALT activation, the first defensive barrier of our body [41,42], with subsequent activation of all local immuno-inflammatory responses [36-45].
The latter is due probably to “psuedoischemia submucosa”, shown by the Rhino-fibroscopy technique. These findings could represent further evidence to support a correlation between the presence of this peculiar lymphocyte and the active or previous infection by SARS-CoV-2, but also a marker of the possible persistence of viral damages at nasal mucosa, even after the recovery from the disease (Long COVID syndrome). Nasal cytology is a non-invasive and easy-to-perform method, that, supported by the results of this study, could have a crucial significance for the monitoring of this viral disease; in fact, it can be performed not only in hospitals but also in medical practices. Additional follow-up studies of SARS-CoV-2 patients could deeply investigate the lymphocyte typing of the second level.
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, Zhao X, Huang B, Shi W, Lu R, Niu P, Zhan F, Ma X, Wang D, Xu W, Wu G, Gao GF, Tan W; China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med. 2020 Feb 20;382(8):727-733. doi: 10.1056/NEJMoa2001017. Epub 2020 Jan 24. PMID: 31978945; PMCID: PMC7092803.
- Sungnak W, Huang N, Bécavin C, Berg M, Queen R, Litvinukova M, Talavera-López C, Maatz H, Reichart D, Sampaziotis F, Worlock KB, Yoshida M, Barnes JL; HCA Lung Biological Network. SARS-CoV-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes. Nat Med. 2020 May;26(5):681-687. doi: 10.1038/s41591-020-0868-6. Epub 2020 Apr 23. PMID: 32327758; PMCID: PMC8637938.
- Flemming A. Poor nasal immunity can lead to severe COVID-19. Nat Rev Immunol. 2021 Sep;21(9):547. doi: 10.1038/s41577-021-00610-2. PMID: 34376831; PMCID: PMC8353604.
- Xydakis MS, Dehgani-Mobaraki P, Holbrook EH, Geisthoff UW, Bauer C, Hautefort C, Herman P, Manley GT, Lyon DM, Hopkins C. Smell and taste dysfunction in patients with COVID-19. Lancet Infect Dis. 2020 Sep;20(9):1015-1016. doi: 10.1016/S1473-3099(20)30293-0. Epub 2020 Apr 15. PMID: 32304629; PMCID: PMC7159875.
- Doyle WJ, Gentile DA, Skoner DP. Viral and bacterial rhinitis. Clin Allergy Immunol. 2007;19:177-95. PMID: 17153013.
- Gelardi M, Ciprandi G. Ciliocytophthoria of nasal epithelial cells after viral infection: a sign of suffering cell. Acta Biomed. 2019 Jan 14;90(2-S):7–9. doi: 10.23750/abm.v90i2-S.8103. PMID: 30715030; PMCID: PMC6502078.
- Aslani FS, Khademi B, Yeganeh F, Kumar PV, Bedayat GR. Nasal cytobrush cytology: evaluation of the hyperchromatic supranuclear stria. Acta Cytol. 2006 Jul-Aug;50(4):430-4. doi: 10.1159/000325987. PMID: 16901009.
- Gelardi M, Cassano P, Cassano M, Fiorella ML. Nasal cytology: description of a hyperchromatic supranuclear stria as a possible marker for the anatomical and functional integrity of the ciliated cell. Am J Rhinol. 2003 Sep-Oct;17(5):263-8. PMID: 14599129.
- Gelardi M, Notargiacomo M, Trecca EMC, Cassano M, Ciprandi G. COVID-19 and Nasal Cytobrush Cytology. Acta Cytol. 2020;64(4):397-398. doi: 10.1159/000508768. Epub 2020 May 26. PMID: 32454497; PMCID: PMC7316649.
- Ahn JH, Kim J, Hong SP, Choi SY, Yang MJ, Ju YS, Kim YT, Kim HM, Rahman MDT, Chung MK, Hong SD, Bae H, Lee CS, Koh GY. Nasal ciliated cells are primary targets for SARS-CoV-2 replication in the early stage of COVID-19. J Clin Invest. 2021 Jul 1;131(13):e148517. doi: 10.1172/JCI148517. PMID: 34003804; PMCID: PMC8245175.
- Gelardi M. Atlas of nasalcytology for the DifferentialDiagnosis of NasalDiseases, II ed. Milano, Ed. Ermes. 2012; 92.
- El Jamal SM, Salib C, Stock A, Uriarte-Haparnas NI, Glicksberg BS, Teruya-Feldstein J, Dembitzer FR, Nadkarni GN, Firpo-Betancourt A. Atypical lymphocyte morphology in SARS-CoV-2 infection. Pathol Res Pract. 2020 Sep;216(9):153063. doi: 10.1016/j.prp.2020.153063. Epub 2020 Jun 10. PMID: 32825937; PMCID: PMC7284261.
- Nazarullah A, Liang C, Villarreal A, Higgins RA, Mais DD. Peripheral Blood Examination Findings in SARS-CoV-2 Infection. Am J Clin Pathol. 2020 Aug 5;154(3):319-329. doi: 10.1093/ajcp/aqaa108. PMID: 32756872; PMCID: PMC7454310.
- Weinberg SE, Behdad A, Ji P. Atypical lymphocytes in peripheral blood of patients with COVID-19. Br J Haematol. 2020 Jul;190(1):36-39. doi: 10.1111/bjh.16848. Epub 2020 Jun 2. PMID: 32420613; PMCID: PMC7276903.
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, Zhao X, Huang B, Shi W, Lu R, Niu P, Zhan F, Ma X, Wang D, Xu W, Wu G, Gao GF, Tan W; China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med. 2020 Feb 20;382(8):727-733. doi: 10.1056/NEJMoa2001017. Epub 2020 Jan 24. PMID: 31978945; PMCID: PMC7092803.
- Huang C, Wang Y, Li X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497-506
- Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, Qiu Y, Wang J, Liu Y, Wei Y, Xia J, Yu T, Zhang X, Zhang L. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020 Feb 15;395(10223):507-513. doi: 10.1016/S0140-6736(20)30211-7. Epub 2020 Jan 30. PMID: 32007143; PMCID: PMC7135076.
- Rodriguez-Morales AJ, Cardona-Ospina JA, Gutiérrez-Ocampo E, Villamizar-Peña R, Holguin-Rivera Y, Escalera-Antezana JP, Alvarado-Arnez LE, Bonilla-Aldana DK, Franco-Paredes C, Henao-Martinez AF, Paniz-Mondolfi A, Lagos-Grisales GJ, Ramírez-Vallejo E, Suárez JA, Zambrano LI, Villamil-Gómez WE, Balbin-Ramon GJ, Rabaan AA, Harapan H, Dhama K, Nishiura H, Kataoka H, Ahmad T, Sah R; Latin American Network of Coronavirus Disease 2019-COVID-19 Research (LANCOVID-19). Electronic address: https://www.lancovid.org. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med Infect Dis. 2020 Mar-Apr;34:101623. doi: 10.1016/j.tmaid.2020.101623. Epub 2020 Mar 13. PMID: 32179124; PMCID: PMC7102608.
- Chong VCL, Lim KGE, Fan BE, Chan SSW, Ong KH, Kuperan P. Reactive lymphocytes in patients with COVID-19. Br J Haematol. 2020 Jun;189(5):844. doi: 10.1111/bjh.16690. Epub 2020 May 5. PMID: 32297330; PMCID: PMC7262365.
- Zini G, Bellesi S, Ramundo F, d'Onofrio G. Morphological anomalies of circulating blood cells in COVID-19. Am J Hematol. 2020 Jul;95(7):870-872. doi: 10.1002/ajh.25824. Epub 2020 Apr 22. PMID: 32279346; PMCID: PMC7262044.
- Caruso AA, Prete SD, Marasco D, Salzano J, Naviglio D, Gallo M, Ferrara L. Epstein - Barr virus Infection Documented by Lymphocyte Studyafter Nasal Scraping: Case Report., JOSR Journal of Dental and Medical Sciences (IOSR-JDMS). 2018; 17:7; 72-74.
- Gallo O, Locatello LG, Mazzoni A, Novelli L, Annunziato F. The central role of the nasal microenvironment in the transmission, modulation, and clinical progression of SARS-CoV-2 infection. Mucosal Immunol. 2021 Mar;14(2):305-316. doi: 10.1038/s41385-020-00359-2. Epub 2020 Nov 26. PMID: 33244161; PMCID: PMC7690066.
- Ziegler CGK, Miao VN, Owings AH, Navia AW, Tang Y, Bromley JD, Lotfy P, Sloan M, Laird H, Williams HB, George M, Drake RS, Christian T, Parker A, Sindel CB, Burger MW, Pride Y, Hasan M, Abraham GE 3rd, Senitko M, Robinson TO, Shalek AK, Glover SC, Horwitz BH, Ordovas-Montanes J. Impairedlocalintrinsicimmunity to SARS-CoV-2 infection in severe COVID-19. bioRxiv [Preprint]. 2021 Feb 20:2021.02.20.431155. doi: 10.1101/2021.02.20.431155. Update in: Cell. 2021 Jul 23;: PMID: 33619488; PMCID: PMC7899452.
- Foldes D, Hinton R, Arami S, Bain BJ. Plasmacytoid lymphocytes in SARS-CoV-2 infection (Covid-19). Am J Hematol. 2020 Jul;95(7):861-862. doi: 10.1002/ajh.25834. Epub 2020 Apr 28. PMID: 32298486; PMCID: PMC7262137.
- Gérard D, Henry S, Thomas B. SARS-CoV-2: a new aetiology for atypical lymphocytes. Br J Haematol. 2020 Jun;189(5):845. doi: 10.1111/bjh.16730. Epub 2020 May 14. PMID: 32311762; PMCID: PMC7264674.
- Wang F, Nie J, Wang H, Zhao Q, Xiong Y, Deng L, Song S, Ma Z, Mo P, Zhang Y. Characteristics of Peripheral Lymphocyte Subset Alteration in COVID-19 Pneumonia. J Infect Dis. 2020 May 11;221(11):1762-1769. doi: 10.1093/infdis/jiaa150. PMID: 32227123; PMCID: PMC7184346.
- Weinberg SE, Behdad A, Ji P. Atypical lymphocytes in peripheral blood of patients with COVID-19. Br J Haematol. 2020 Jul;190(1):36-39. doi: 10.1111/bjh.16848. Epub 2020 Jun 2. PMID: 32420613; PMCID: PMC7276903.
- Chng WJ, Lai HC, Earnest A, Kuperan P. Haematological parameters in severe acute respiratory syndrome. Clin Lab Haematol. 2005 Feb;27(1):15-20. doi: 10.1111/j.1365-2257.2004.00652.x. PMID: 15686503; PMCID: PMC7165508.
- Lee N, Hui D, Wu A, Chan P, Cameron P, Joynt GM, Ahuja A, Yung MY, Leung CB, To KF, Lui SF, Szeto CC, Chung S, Sung JJ. A major outbreak of severe acute respiratory syndrome in Hong Kong. N Engl J Med. 2003 May 15;348(20):1986-94. doi: 10.1056/NEJMoa030685. Epub 2003 Apr 7. PMID: 12682352.
- Gawoski JM, Ooi WW. Dengue fever mimicking plasma cell leukemia. Arch Pathol Lab Med. 2003 Aug;127(8):1026-7. doi: 10.5858/2003-127-1026-DFMPCL. PMID: 12873179.
- Hadjadj J, Yatim N, Barnabei L, Corneau A, Boussier J, Smith N, Péré H, Charbit B, Bondet V, Chenevier-Gobeaux C, Breillat P, Carlier N, Gauzit R, Morbieu C, Pène F, Marin N, Roche N, Szwebel TA, Merkling SH, Treluyer JM, Veyer D, Mouthon L, Blanc C, Tharaux PL, Rozenberg F, Fischer A, Duffy D, Rieux-Laucat F, Kernéis S, Terrier B. Impaired type I interferon activity and inflammatory responses in severe COVID-19 patients. Science. 2020 Aug 7;369(6504):718-724. doi: 10.1126/science.abc6027. Epub 2020 Jul 13. PMID: 32661059; PMCID: PMC7402632.
- Galani IE, Rovina N, Lampropoulou V, Triantafyllia V, Manioudaki M, Pavlos E, Koukaki E, Fragkou PC, Panou V, Rapti V, Koltsida O, Mentis A, Koulouris N, Tsiodras S, Koutsoukou A, Andreakos E. Untuned antiviral immunity in COVID-19 revealed by temporal type I/III interferon patterns and flu comparison. Nat Immunol. 2021 Jan;22(1):32-40. doi: 10.1038/s41590-020-00840-x. Epub 2020 Dec 4. PMID: 33277638.
- Kusnadi A, Ramírez-Suástegui C, Fajardo V, Chee SJ, Meckiff BJ, Simon H, Pelosi E, Seumois G, Ay F, Vijayanand P, Ottensmeier CH. Severely ill COVID-19 patients display impaired exhaustion features in SARS-CoV-2-reactive CD8+ T cells. Sci Immunol. 2021 Jan 21;6(55):eabe4782. doi: 10.1126/sciimmunol.abe4782. PMID: 33478949; PMCID: PMC8101257.
- Liu C, Martins AJ, Lau WW, Rachmaninoff N, Chen J, Imberti L, Mostaghimi D, Fink DL, Burbelo PD, Dobbs K, Delmonte OM, Bansal N, Failla L, Sottini A, Quiros-Roldan E, Han KL, Sellers BA, Cheung F, Sparks R, Chun TW, Moir S, Lionakis MS; NIAID COVID Consortium; COVID Clinicians; Rossi C, Su HC, Kuhns DB, Cohen JI, Notarangelo LD, Tsang JS. Time-resolved systems immunology reveals a late juncture linked to fatal COVID-19. Cell. 2021 Apr 1;184(7):1836-1857.e22. doi: 10.1016/j.cell.2021.02.018. Epub 2021 Feb 10. PMID: 33713619; PMCID: PMC7874909.
- Lucas C, Wong P, Klein J, Castro TBR, Silva J, Sundaram M, Ellingson MK, Mao T, Oh JE, Israelow B. Yale IMPACT Team. Longitudinalanalysesrevealimmunologicalmisfiring in severe COVID-19. Nature. 2020; 584, 463–469.
- Mathew, D., Giles, J.R., Baxter, A.E., Oldridge, D.A., Greenplate, A.R., Wu, J.E., Alanio, C., Kuri-Cervantes, L., Pampena, M.B., D’Andrea, K., et al.; UPenn, COVID Processing Unit (2020). Deep immune profiling of COVID-19 patientsrevealsdistinctimmunotypes with therapeuticimplications. Science 369, 80.
- Schulte-Schrepping J, Reusch N, Paclik D, Baßler K, Schlickeiser S, Zhang B, Kra¨ mer B, Krammer T, Brumhard S, Bonaguro L. DeutscheCOVID-19 OMICS Initiative (DeCOI). Severe COVID-19 IsMarked by a DysregulatedMyeloid Cell Compartment. Cell. 2020; 182:1419–1440.e23.
- Stephenson E, Reynolds G, Botting RA, Calero-Nieto FJ, Morgan M, Tuong ZK, Bach K, Sungnak W, Worlock KB, Yoshida M. The cellular immune response to COVID-19 deciphered by single cell multi-omicsacrossthree UK centres. (medRxiv). 2021. https://doi.org/10.1101/2021.01.13.21249725.
- Su Y, Chen D, Yuan D, Lausted C, Choi J, Dai CL, Voillet V, Duvvuri VR, Scherler K, Troisch P, Baloni P, Qin G, Smith B, Kornilov SA, Rostomily C, Xu A, Li J, Dong S, Rothchild A, Zhou J, Murray K, Edmark R, Hong S, Heath JE, Earls J, Zhang R, Xie J, Li S, Roper R, Jones L, Zhou Y, Rowen L, Liu R, Mackay S, O'Mahony DS, Dale CR, Wallick JA, Algren HA, Zager MA; ISB-Swedish COVID19 Biobanking Unit; Wei W, Price ND, Huang S, Subramanian N, Wang K, Magis AT, Hadlock JJ, Hood L, Aderem A, Bluestone JA, Lanier LL, Greenberg PD, Gottardo R, Davis MM, Goldman JD, Heath JR. Multi-Omics Resolves a Sharp Disease-State Shift between Mild and Moderate COVID-19. Cell. 2020 Dec 10;183(6):1479-1495.e20. doi: 10.1016/j.cell.2020.10.037. Epub 2020 Oct 28. PMID: 33171100; PMCID: PMC7598382.
- Wilk AJ, Rustagi A, Zhao NQ, Roque J, Martínez-Colón GJ, McKechnie JL, Ivison GT, Ranganath T, Vergara R, Hollis T, Simpson LJ, Grant P, Subramanian A, Rogers AJ, Blish CA. A single-cell atlas of the peripheral immune response in patients with severe COVID-19. Nat Med. 2020 Jul;26(7):1070-1076. doi: 10.1038/s41591-020-0944-y. Epub 2020 Jun 8. PMID: 32514174; PMCID: PMC7382903.
- Lehtinen MJ, Hibberd AA, Männikkö S, Yeung N, Kauko T, Forssten S, Lehtoranta L, Lahtinen SJ, Stahl B, Lyra A, Turner RB. Nasal microbiota clusters associate with inflammatory response, viral load, and symptom severity in experimental rhinovirus challenge. Sci Rep. 2018 Jul 30;8(1):11411. doi: 10.1038/s41598-018-29793-w. PMID: 30061588; PMCID: PMC6065324.
- Rose MA, Zielen S, Baumann U. Mucosal immunity and nasal influenza vaccination. Expert Rev Vaccines. 2012 May;11(5):595-607. doi: 10.1586/erv.12.31. PMID: 22827245.